|
|
 |
|
|
Low sugar population, health testing, book reviews
|
|
|
LSP the evidence that they don’t get
CAWD:
Combine with 1-B-LSP intro
Mystery:
This book is
about solving why those
populations on a low sugar diet (LSPs) have a different set of illnesses. It is about what has been known since 1982 called conditions
associated with the western diet (CAWD),
and before that as conditions of civilization,
and prior as conditions of affluence. It arrives at the cause, fructose, and how
through fructosylation (fructation) it damages the mitochondria (MTD), and when
consumed significantly
above what cellular repair system can repair, the altered functions of the
cells throughout the body increase the risks for all the CAWD, and especially
among the elderly in what is known as age
related conditions. Since
the seminal work by Burkett and Trowel in 1981, the science solving that
mystery has made an incontrovertible case against fructose. The second
of 6 Sections is on sugars. The
third section is on the mitochondria, which fructose “modifies” through the Trojan
horses of proteins and polyunsaturated fats (PUFAs): it bonds to them in
a process of fructation (also labeled fructosylation) in the cytosol, and some
of those damaged molecules are transported into the mitochondria a topic in
Section 3, which is devoted to the mitochondria and its altered performance,
most significantly is the reduced production of ATP, the causal factor for
insulin resistance (IR) in the
liver. Section 4 names what I considered
the most significant changes the
damage goods cause operating through a diminished production of ATP and other
chemicals produced by the mitochondria.
On the big demon list is a reduced production of collagen, sensitivity
to uric acid, and a reduced rate of autophagy (RRA). RRA explains why low
sugar populations are resistant to, for example the effect of cigarettes (the
degree correlates to the percentage of those who life-long limit their sugar to
under 24 grams a day (WHO’s dietary recommendation for sugar intake for women).
Section
5 is on those conditions that are called age related health conditions but
are more accurately called conditions associated with the western diet (CAWD) since they are nearly unknown
among the low sugar populations (LSPs).
Thus by Section 4 is set out the cause
for our health disaster, and the association between mitochondrial dysfunction
(MTDD) and the conditions, the topic
for section 5. And since most readers
would be interested in what to do repair our fructose damage mitochondria and
the consequences there from, as a Benthamite (utilitarian) I am morally
obligated to write a Section 6 on
what to do. Simply limiting sugar to 24
grams a day will only very slow promote healing among adults, much quicker
among children, and at a moderate rate among young adults. There are ways to
double and quadruple that
rate, and this is what Section 6 is about.
Oh,
and as a Benthamite I am also obligated to set the record straight concerning
tobacco science and its consequence.
Thus many bromides [truths that on the shelf of time are stable] that
are engraved in textbooks and taught by key opinion leaders (KOLs) and their
dupes; these bromides
will be dumped into my acid bath of basic science. The foundation of this book,
and thus the
bath is to piece together into a sold fabric the pieces of science that answer
the basic questions of why we get what are now as conditions associated with
the western diet, and the LSPs don’t get them.
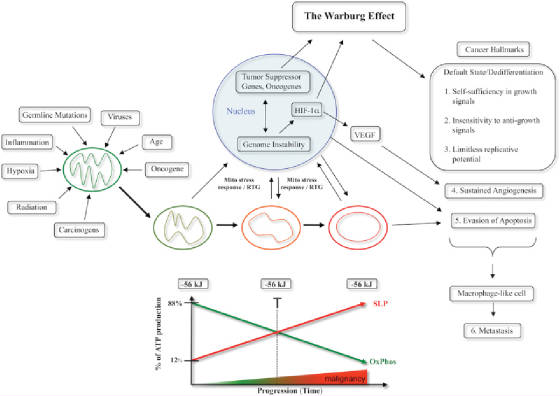
The test is the modus operandi, the why is this happening. Why do we
get cancer, and they don’t? Why is fructose very different than
glucose? Why does the LSPs mitochondria
outperform the mitochondria of the HSPs?
Why does this difference effect health, and how? The answers are
there is journal articles,
thousands of journal articles, many of them tangent, and a few seminal covering
a large area of research. I let the
journal speak. This
is more than solving a mystery, it is also about wellness. The amount of harmful
bromide spread as
healthful upon the minds of physicians, dieticians, and the public by KOLS and
their dupes, has created is exposed then in Section 6, there is what to do that
promotes healing.
2. CAWD
I am not
the first to see the association of MTD dysfunction and CAWD: A wide range of seemingly unrelated
disorders, such as schizophrenia,
bipolar disease, dementia, Alzheimer's disease, epilepsy, migraine headaches,
strokes, neuropathic pain, Parkinson's disease, ataxia, transient ischemic
attack, cardiomyopathy, coronary artery disease, chronic fatigue
syndrome, fibromyalgia, retinitis pigmentosa, diabetes, hepatitis C,
and primary biliary
cirrhosis,
have underlying pathophysiological mechanisms
in common, namely reactive oxygen species (ROS)
production, the accumulation of mitochondrial DNA (mtDNA)
damage, resulting in mitochondrial dysfunction—link 2007 .
Insulin
resistance is a result of two complimentary effects, ones is that the damage to
MTD causes both reduced size of MTD and reduced absorption of and metabolism of
glucose (and presumable fructose and galactose which are also metabolized in
MTD. A 2006
study found among other things: glycogen synthesis
was decreased by over
50% in patients with type 2 diabetes. That study also found consistent with
population studies that the children of diabetics have similar reduction in
metabolism of glucose: “Further analysis
has found that the reduction in mitochondrial function in the insulin-resistant
offspring can be mostly attributed to reductions in mitochondrial density.” This finding is supported by another which
measured the size of MTD of three groups of 10 each, lean, slightly obese and
t2d.
3. Biomarkers of LSPs:
What is normal biomarkers for those on the
western diet, isn’t for LSPs on a paleo diet

Table 2: Systolic
blood pressure (SBP) and diastolic blood pressure (DBP)
at age 40–60 years in hunter–gatherers and horticulturalists (mm Hg) 26,
67–69
|
Population -----
|
Men
|
|
Women -
|
|
|
|
SBP---- -
|
DBP-- ----
|
SBP
|
DBP -----
|
|
|
|
|
|
|
|
Bushman
|
108
|
63
|
118
|
71
|
|
Yanomamo
|
104
|
65
|
102
|
68
|
|
Xingu
|
107
|
68
|
102
|
63
|
|
Kitava
|
113
|
71
|
121
|
71
|
Table 3: Systolic
blood pressure and diastolic
blood pressure in Yanomamo Indians 69.
|
Age years --------
|
Men -----------
|
Women------
|
|
0-9
|
93/59
|
96/62
|
|
10-19
|
108/67
|
105/65
|
|
20-29
|
108/69
|
100/63
|
|
30-39
|
106/69
|
100/63
|
|
40-49
|
107/67
|
98/62
|
|
50 +
|
100/64
|
106/64
|
Figure 1, Fasting
plasma insulin (IU/mL) in Kitava horticulturists (first
number) versus healthy Swedes (second number).74 Transposed
from graph by JK
|
Men 25-39
|
40-59
|
60-74
|
|
Women 25-39
|
40-59
|
60-74
|
|
3.9 vs 5.7
|
3.5 vs 6.85
|
3.55 vs 7.65
|
|
3.5 vs 6.2
|
3.85 vs 3.9
|
3.8 vs 7.25
|
Figure 3, Fasting
plasma leptin (ng/mL) in Kitava horticulturalists versus
healthy Swedes. 92
|
Men <40
|
40-59
|
60 +
|
|
Women < 40
|
40-59
|
60 +
|
|
1.7 vs 3.4
|
3.5 vs 5.2
|
3.7 vs 7.2
|
|
5.95 vs 11.4
|
3.2 vs 14.1
|
3.95 vs 19.1
|
Figure 4 Fasting plasma leptin
(ng/mL) in Ache Indians versus
American marathon runners.83
Ache (Axe people) are indigenous hunter-gatherers of eastern Paraguay.
|
Ache
|
American
runners
|
|
1.15
|
2.20
|
Systematic
recording of dietary intake while living in the forest entirely off wild foods
suggests that about 80% of their energy in the diet comes from meat, 10% from
palm starch and hearts, 10% from insect larva and honey, and 1% from fruits.
Total energy intake is approximately 2700 kcal per person daily.[1]
Figure 7, Maximum
oxygen consumption in various populations (mL/kg/min). 67
|
Lufas
|
Maasai
|
Eskimos
|
Lapps
|
Warao
|
IKung
|
Average American
|
|
67
|
58.5
|
57
|
53
|
51
|
49
|
42
|
Note, JK: the IKung are desert dwellers in South
Africa and the Warao live in costal Jungle regions of Northern South America
all of which the temperature limits physical excursion; while the Lapps and
Eskimos for most of the year can’t breathe deeply. The Maasai live
on the plains of Kenyan and Tanzania. The Lufas, I
couldn’t find a reference to, the link
#97 to the abstract didn’t
reference oxygen consumption, and the
full article is not available for free. Oxygen
consumption is associated with,
cardiovascular fitness. After insulin resistance, fitness is the
best marker for health/longevity——link to senior runners.
Cardiovascular fitness is of all measurement the best predictor health
and quality of life. So why is there so
a difference in all of this markers for health of LSPs and HSPs. Figure 1 and
4 contain the answer, IR. Children on the western diet develop IR. Many by comparison to the LSPs are born with
IR. A mother with IR pass on through
fetal environment IR. Her elevated glucose causes cellular responses that
affect the number of receptors for the transport of glucose into cells and
other cellular functions. It is a fetal
adaptation to the dietary environment the child will be exposed to. These changes
on a cellular level or further
established by the frequently consumption of excessive sugar. What I predict
is that at some point, even
with physical training and change of diet, obtaining the levels of insulin and
leptin in figures 1 & 4 will not be possible. My guess would be by the 25th
year—could well be in the teen years.
4. Defective mitochondria:
What is driving the damage to the
mitochondria. The literature finds 3
causes: oxidative stress from the
reactive chemical created in metabolism, in addition there is the role of uric
acid produced during the metabolism of fructose in the mitochondria, there is
fructosylation, and with damage to the mitochondria the repair systems of the
mitochondria are not functioning at optimal levels. Evidence from defective
mitochondria comes
from lower use of oxygen and smaller size in those with type 2 diabetes--at 2005, 2006. “A reduced basal ADP-stimulated and maximal mitochondrial
respiratory
capacity underlies the reduction in in vivo mitochondrial function, independent
of mitochondrial content [number of mitochondria]. A reduced capacity at both
the level of the
electron transport chain and phosphorylation system underlies this impaired
mitochondrial capacity [less ATP molecules]”--at 2008. As maintained those with IR in
the liver which is caused by the
high fructose diet will develop in the liver and later in other tissues
defective mitochondria similar the diabetic but to a lesser degree. This will
causes a decrease in the
production of ATP through the Krebs cycle, and as a consequence an increase in
cellular and serum glucose. In
the liver and conversion rate of
glucose to glycogen and the production of ATP has decrease due to defective
mitochondria and the effects of inflammation caused by a fatty liver, thus
slowing the utilization of glucose and raising serum glucose, the hallmark of IR—see
2008
and 2011.
Cells throughout the body already load with
glucose become resistant to the uptake of more glucose as the liver’s functions
decline. Through a feedback mechanism these body cells become resistant to the
uptake of more glucose. Added to this is the Crabtree effect: a high level of
glucose down regulates glucose
metabolism (inhibition of respiration), “that effect was strongly antagonized
by fructose 1,6-bisphosphate (F16bp). . . .
as able to inhibit mitochondrial respiration. . .” [2] This
combination of factors explains the development of insulin resistance in
tissues besides the liver.
Fructose
has a very low insulin index because over 95% is taken to the liver by the
hepatic portal vein where it is phosphorylated there thus making it incapable
of passing out of the liver like glucose--Wiki.
invisible to insulin by being taken from the
serum on first pass from the small intestines via the hepatic portal vein to
the liver. This explains why fructose
though invisible to insulin, has a glycemic index (which measures glucose
uptake from foods) of fructose is between 19 to 23, while glucose is rated at
100, and sucrose at 60 (thus not 50). The
rise in insulin is because of the slower uptake
of glucose through the GLUT-5 transport system into the hepatocytes.
“Perturbations in the regulation of glucose
and lipid metabolism are both involved in the insulin resistance in skeletal
muscle in obesity and type 2 diabetes (2,3). Previously, our
laboratory (30) as well as others (31) have observed that
the severity of skeletal muscle insulin resistance in type 2 diabetes and
obesity is related to diminished activity of oxidative enzymes. In addition,
accumulation of triglycerides in skeletal muscle is also correlated with the
severity of insulin resistance and with diminished oxidative enzyme activity in
these disorders(23) [not causal] . . .
The mitochondria area was reduced by ~35% in type 2 diabetes and obesity.” at
2002. Size and shape of mitochondria are strong
associated with compromised functioning of the mitochondria—see for example the
work of Nobel Laureate Otto Warburg.
Research is needed to find out if this change also occurs with IR.

Decline
in skeletal muscle mitochondrial function with aging humans[3]
[1] Wiki, 12/18 Ache https://en.wikipedia.org/wiki/Ach%C3%A9. The
article’s discussion of their diet puzzles on why the men prefer to hunt rather
than gather food for which coconuts are plentiful and supplies 25% more energy
per hour of labor than hunting. I aver
that hunting reduces boredom more than gathering foods such as coconuts. Given this it explains why another article
finds that the average for hunter-gatherers is 60% of calories from animals and
insects.
[2] Kelley, David,
Jing He, et al Oct 2002, Dysfunction of
Mitochondria in Human Skeletal Muscle in Type 2 Diabetes
[3] Kevin
Short, Maureen Bigelow, et al, April 2005, Decline
in skeletal muscle mitochondrial function with aging humans
|
|
|
Review of Burkett & Trowell -- include
WESTERN DISEASES:
THEIR EMERGENCE AND PREVENTION. By H.C. Trowell
and D.P. Burkett
Burkitt.
Cambridge, MA, Harvard University
Press, 1981. 456 pp.
$40.00.
During travels through
developing and industrialized
countries in the West
Pacific, Far East, and Central America, I
often wondered about the
state of
health of these peoples and those in similar countries
around
the world. I was especially curious about
the prevalence of chronic
non-infectious diseases and how these were
related to culture, environment,
diet, and personal
health practices. Furthermore,
I was intrigued
about the extent to which Western
acculturation directly or indirectly
affected health.
These questions are now answered on
a global basis in this book edited
by two eminent physicians,
H.C. Trowell and D.P.
Burkitt. I applaud their efforts and those of the contributors in presenting current
information on this timely and
significant aspect of international health and epidemiology.
As is succinctly
stated in their preface, "this book attempts
to discuss
the commoner diseases of civilization." In essence, these diseases are
ones felt by the editors
to be
characteristic of modern Western
industrialized societies:
metabolic and cardiovascular diseases (e.g., coronary artery disease, hypertension, diabetes
mellitus, cerebrovascular
disorders); intestinal diseases (e.g., appendicitis, diverticular disease, cancer, hemorrhoids, polyps, constipation);
and a variety of
others, including
nephrolithiasis, gout,
pernicious anemia,
thyrotoxicosis, and breast and lung cancer.
The
major chapters in the book study
several specific populations from
all corners of the earth. They
are collected in sections
under the concepts of hunter-gatherers, peasant-agriculturists,
migrants and mixed ethnic
groups, and
the Far East. The people described include Inuit Eskimos, Australian
aborigines, Pacific Island groups,
South African
populations, Hawaiian ethnic groups,
and the population
of Taiwan and China. The chapters
are thorough and well-written, with
numerous and current references. The 34 contributors,
of whom the majority are physicians, have
had extensive experience living and working with
these populations. In
each chapter, discussions
cover population
demographics, cultural aspects of the
diet, and important studies on
disease-specific morbidity
and mortality
data. A common thread running through
all of the chapters is the role of
diet (carbohydrate, fat,
fiber, and protein components) and known health
risk factors (smoking, sedentary living, alcohol consumption,
stress concomitants,
and individual susceptibility)
as associated
factors in the epidemiology
of these diseases. Topics are presented
in an informative manner for the reader to
consider, without biased "breast-beating"
over conjectured dogmas. Another section of chapters
is concerned with the international epidemiology
and environmental aspects
of certain important
diseases, including multiple sclerosis,
cancer, and the
arthritides. The current state
of the art
in the treatment and prevention
of cardiovascular diseases,
intestinal disorders, and
diabetes mellitus is also examined. There are only two
shortcomings of this book,
but they are inherent in
its design and do not detract from its purpose.
In some instances, the available orbidity
and data are limited and
are not able to
be broken down into specific rates,
i.e., by age group. Second, the subject of psychiatric diseases is not covered;
however, this would entail a separate text.
Western Diseases: Their
Emergence and Prevention
stands on its own merits
as a welcomed and necessary reference for
those
involved in the fields of international health and epidemiology. I
also highly recommend this
book to anyone who anticipates working in
the fields of overseas health care or
exploration medicine.
MARK L. DEMBERT
Department of
Epidemiology and
Public Health
Yale University School of Medicine
^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^^
https://www.lrb.co.uk/v03/n24/thomas-mckeown/the-burden-of-prudence-industrialisation-and-disease
The Burden of
Prudence – Industrialisation and Disease
Thomas McKeown
Hugh Trowell and Denis
Burkitt are a distinguished physician and surgeon who have spent most of their
professional lives in Africa; with T.L. Cleave and G.D. Campbell, they have
probably contributed more than anyone else to our understanding of the relation
between the health problems of developed and developing countries. In Western
Diseases they bring together reports by 34 contributors, who
describe their experience of changes in the pattern of disease in several
countries as Westernisation occurs. There are four main lines of evidence,
which the editors admit are not all equally secure. 1. Until recently many of
the non-communicable diseases now predominant in the West were uncommon or
absent in hunter-gatherers and peasant agriculturists. 2. When these
populations change from their traditional ways of life to those of the
developed countries, they begin to exhibit the Western pattern of disease. 3.
The incidence of some of the diseases has declined in Western populations which
have reversed certain features of their lifestyle to bring it closer to that of
peasant agriculturists. 4. Of the multiple influences responsible for the
Western pattern of disease, dietary changes are probably the most important.
The full text of this book
review is only available to subscribers of the London Review of Books.
|
|
|
|
|
|
|
|
|
|
|
|
|