|
An understanding the role of atherosclerosis in the development of CVD
is necessary for rational, evidence-based heart choices. Atherosclerosis
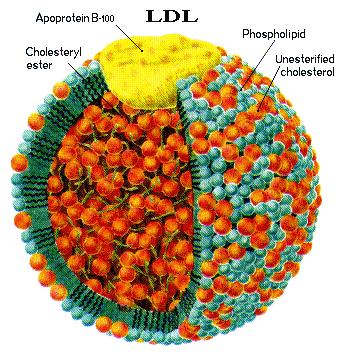
is caused by oxidative damage to the
cholesterol contained within the LDL that is in
the lumen of arteries. [See LDL illustraton] This causes an immune response by
T-lymphocytes and macrophages (both types of white blood cells) that starts atherogenesis.
This response results in the formation of
unstable young plaque within the lumen of arteries which over a period of
several years will become harden (stable plaque). The unstable plaque causes
over 90% of MIs
(myocardial infarctions, heart attacks) & 85% of strokes. (Retain this essential
relationship.) This analysis has been accepted based upon a
large body of experimental and epidemiological (population studies)
evidence.
Atheroma: “The atheroma
(accumulation & swelling in
an artery wall) consists of LDL [see illustration],
calcium, fibrous connective tissues, T-lymphocytes macrophages, and pathogens. While in the
early stages, based on gross appearance, have traditionally been termed fatty streaks by pathologists, they are not composed of
fat cells ( adipose cells), but are accumulations of
white blood cells, especially macrophages, that have taken up
oxidized low-density lipoprotein (LDL). After they accumulate large amounts of
cytoplasmic membranes (with associated high cholesterol content) the
macrophages are called foam cells. When foam cells die,
their contents are released, which attracts more macrophages
Coronary artery
disease (CAD), atherosclerotic heart disease, cardiovascular
disease (CVD) are caused by atherosclerosis
(AS) affects coronary arteries and
thus the blood supply to the heart muscle. “Atherosclerosis is the most common
type of heart disease and cause of heart attacks.[1] The disease is caused by plaque building up along the
inner walls of the arteries of the heart, which narrows the arteries and restricts blood flow to the
heart. It is the leading cause of death worldwide.[1]
After decades of progression, some of the atheromatous plaques may rupture
and (along with the activation of the blood clotting system) start limiting blood flow to the heart muscle. The disease is the
most common cause of sudden death,[2] and the leading cause of death over the age
of 20 years.[3] Most
commonly,
unstable young plaque ruptures and may lead to an acute myocardial infarction (AMI). Cholesterol is delivered into the
vessel wall by cholesterol-containing low-density lipoprotein (LDL)
particles. To attract and stimulate macrophages (a type of white cell), the
cholesterol must be released from the LDL particles and oxidized, a key step in
the ongoing inflammatory process” Wiki. “T-lymphocytes respond to the oxidized LDL by activating
CXC chemokines which attracts macrophages” JCI. “The process
is
worsened if there is insufficient high-density lipoprotein (HDL). The lipoprotein particle [HDL] that removes
cholesterol from tissues and carries it back to the liver. When the macrophages
[type of white blood
cell] engulf a large amount of the oxidized cholesterol [as part of the
disposal process] they are called foam cells because of appearance. In sufficient numbers they form the
fatty streaks of the plaques of atheroma in the innermost layer of the artery
wall. A protective fibrous cap normally
forms between the fatty deposits and the artery lining (the intima).
These capped fatty deposits (now called 'atheromas') produce enzymes
that cause the artery to enlarge over time. Atheromas within the vessel wall
are soft and fragile with little elasticity. Arteries constantly expand and
contract with each heartbeat, i.e., the pulse. In addition, the calcification
deposits between the
outer portion of the atheroma and the muscular wall, as they progress, lead to a loss of
elasticity and stiffening of the artery as a whole” Wiki. The heart responding
to signals of insufficient oxygen pumps blood with more force in order to
supply adequate oxygenated blood to the organs.
Hard, clogged arteries are the principle cause of high blood pressure. The
signal to pump harder is a response of
organs to the lack of oxygen caused by AS.
Hypertension
thus is a trailing result not a cause of AS. The higher risk of ischemic
events (MI and ischemic strokes) is
a result of AS, not of the
co-phenomena of HT [1]. To lower blood pressure does
not significantly affect unstable
plaque the cause of ischemic events.[2]
Macrophages during their cleanup
function weaken the protein matrix and thereby increase the risk for the young
plaque will leak out of the lumen.
As
stated above LDL
plays a key role in AS only when it
has been oxidized by reactive chemicals.
“The same data suggests that only small dense LDL (sdLDL) particles are
able to get behind the cellular monolayer of endothelium [lumen]. LDL particles and their content are
susceptible to oxidation by free radicals,[3] and the risk may be higher while in
the bloodstream. However, LDL particles have a half-life of only a couple of days, and their content
(LDL particles carry cholesterol, cholesteryl esters, and triglycerides from
the liver to the tissues of the body) changes with time. Once inside the vessel
wall, LDL particles
get stuck and their content becomes more prone to oxidation. The damage caused
by the oxidized LDL
molecules triggers a cascade of immune responses which over time can produce an
atheroma…. Atherosclerosis may be caused by an infection of the
vascular smooth muscle cells. For example,
Cytomegalovirus (CMV) infection is also associated with cardiovascular
diseases.[13] In time, as cells die, this leads to
extracellular calcium deposits between the muscular wall and outer portion of
the atheromatous plaques. The
accumulation of calcium leads to a loss of elasticity and stiffening of the
artery as a whole [one cause of HT] “ Wiki. A number of chronic
conditions have been associated with CVD.
Thus women with rheumatoid arthritis have
“double the risk of a heart attacks when compared to women without it… An
infection that starts in the gums, for example, can easily lead bacteria into
the blood-stream that may find fertile ground in a weakened arterial wall and
fan the fires of inflammation there” (Bowden 45). Thus infection is a cause of AS.
The infection vector in the causes of AS consists
of a direct involvement through infection within the artery lumen, and an indirect through chronic
infection. Among chronic infections, the
Helicobacter pylori (the cause for over 80% of ulcers) increase the risk
of MI by 75%. “A number of acute and
chronic infections including: Chlamydophila pneumoniae, lupus erythematosus, influenza,
and Porphyromonas gingivalis [gingivitis] among others
have been linked to atherosclerosis and myocardial infarction” Wiki. “Women with rheumatoid arthritis, a highly
inflammatory condition that primarily affects the joints, wind up having double
the risk of a heart attack…” (Bowden 45).
Within the artery lumen Cytomegalovirus, herpes virus and several
other
pathogens have been found upon examination during autopsy examinations. Thus there are two immune response involved in
AS, one from oxidative damage to LDL,
the other is caused by chronic bacteria and virus infections, of which some are
in the lumen of the artery. Epidemiological studies support their role as
does examination of plaque. Moreover the
test for C-reactive protein (CPR) is
a better predictor of ischemic events in men followed long-term than that of
elevated LDL. CPR is a marker for
infection[4]. This is more evidence of the importance for
reducing the process of oxidative damage to LDL and the inflammation response,
rather than lowering LDL. Thus on this
model the current attempts to prevent the consequences of AS are not addressing
its two major causal factors of immune response and oxidative damage to
LDL.
A review
of the first 50 citation
for “infection + atherosclerosis” found not one article published after 2003 on
infection as a cause for atherosclerosis but for 3 on HIV. A promising area
of research is not being
funded. This follows the business model
of pharma. Pharma profits more from
treating the results of CVD rather
than preventing it: profits come before
people.
Unstable
plaque, the wild card: unstable plaque is fresh,
young plaque that forms within the lumen of an artery. Unstable plaque is why a
person, Al age 60, who has life-long a good lifestyle, has normal blood
pressure and low TC is still at risk
for an ischemic event. Al has in a few sections
of arteries with unstable plaque, and if it leaks he can have an acute ischemic
event. Suppose he has a twin brother,
Herman, who has done life-long, all the risky things: smokes, is obese, and
has developed type II
diabetes. Herman has 10 times the risk
compared to Al for an ischemic event because he has 10 times the amount of
unstable plaque. Al’s unstable plaque
is caused by pathogens in his artery lumen.
If Al’s wife smokes cigarettes he would also be forming plaque from
oxidative damage to LDL. A third cause
is from glycation of lipoproteins in the lumen.
These processes are silent, and why everyone past the age of 30 is at
risk of an ischemic event. However,
women prior menopause, because of the protective effect of estradiol (best of
estrogens), are at 1/10th the risk compared to men for an ischemic
event. (Contra-pharma, post-menopausal
women should take estradiol to promote the cardiovascular protection, but so
far past attempts to find an analog for men have failed.[5])
So
what is the role of dietary
fat?
Given the role of infection and oxidation of
LDL and the lack of evidence that fat causes either of these, the logical
conclusion is that dietary fat and cholesterol are not important. Guidelines
on diets recommend low fat and low
cholesterol, as though fat is involved in the synthesis of cholesterol. This
fits in with pharma’s bad cholesterol
model, but cholesterol is a sterol (a modified steroid) not a fat. The structures
of the two families of organic
chemicals are miles apart. So too is their
production. For cholesterol “Synthesis within the body starts with
one molecule of acetyl CoA and one molecule of acetoacetyl-CoA, which are hydrated to form 3-hydroxy-3-methylglutaryl CoA (HMG-CoA).[34]” Wiki.
“Fats
are triglycerides: triesters of glycerol and any of several fatty acids, Although the words
"oils",
"fats", and "lipids"
are all used to refer to fats, in reality,
fat is a subset of lipid distinguished from other lipids by structure”
Wiki.
Triglycerides are three fatty acids bonded to glycerol. [stick graphs of structures].

Three fat (fatty
acids) molecules
joined at their COOH to 3-OH groups of a glycerol to form triglyceride.

Dietary cholesterol has little effect. Most
ingested
cholesterol is esterified, and esterified cholesterol is poorly absorbed. Moreover
nearly all of the cholesterol is synthesized in the body.[6] “The body also compensates for any absorption
of additional cholesterol by reducing cholesterol synthesis[9] Cholesterol synthesis can also be turned off
when cholesterol levels are high. HMG-CoA reductase [what statins block]
contains both a cytosolic domain (responsible for its catalytic function) and a
membrane domain.” Wiki. In other words, dietary cholesterol
does not
affect blood cholesterol level.
Production is regulated through a homeostatic mechanism involving the
SREBP protein which is activated when the cholesterol level is low and turned
off when high. “SREBP pathway regulates
expression of many genes that control lipid formation and metabolism and body
fuel allocation.” SERBP regulation explains
why most obese people have a high risk high TC.[7] As for MI
risk, obesity is associated with insulin resistance and thus a high level blood
sugar, and this is associated with plaque formation through glycation of sugars--mainly
fructose—that causes oxidative damage to LDL, thus their much higher MI
rate. But pharma misses the causes (prevention is
not in their business plan) and treats cholesterol with statins, its second
most profitable family of drugs (after psychiatric drugs). Thus the official
push for low-fat &
cholesterol diets based on a wrong assumption, or do they work?
“According
to the [started
in the 50s] Farmingham Heart Study, people who consumed the most cholesterol in their diet did
not have any higher blood cholesterol levels than those who consumed the least
amount…. For most people—though not all—the effect of dietary cholesterol on
serum cholesterol is insignificant” (Bowden & Sinatra 31).[8]
So why are the high fat & high cholesterol
diets touted as a major risk factor for CVD?
One reason is that plaque (atheroma) in part
consists of cholesterol and looks fatty.[9] Another reason is in the 50s rabbits fed a cholesterol
rich diet developed AS. (But these
results were not repeated in
animals su ch as rats and baboon that are not herbivores.) Ancel Keys’
Seven-Country Study in the 50s led
to the popular belief that high fat diet led to high level of TC and CVD. Keys actively promoted
the Mediterranean diet. However, years
later Keys reversed his position and stated in 1997: “There’s no
connection whatsoever between
cholesterol in food and cholesterol in blood.
And we’ve known that all along.
Cholesterol in the diet doesn’t matter at all unless you happen to be a
chicken or a rabbit” Bower supra 33. This
was confirmed in the diet component of the Women’s Health Initiative
(WHI): “there was no significant reduction
in the risk of CHD, stroke, or CVD,”
Wiki. “Despite the common belief
that high cholesterol is a
significant risk factor for coronary artery disease, several independent
population studies in healthy adults have shown that low total cholesterol is
associated with cardiovascular and non-cardiac mortality, indicating that high total
cholesterol is not a risk factor in a
healthy population.16 17 18” BMJ 10//22/13. Following
the pattern of marketing studies, researchers were selected to run clinical
trials that had proved their usefulness to pharma in the past. And the
panel for clinical guidelines “were
selected to include experts who would predictable say that … all level of blood
cholesterol in the United States are too high and should be lowered” Bowden 41 quoting
Dr. Michael Oliver on the new guidelines of the National Institute of Health
Consensus Development Conference Statement, December 10-12, 1984. This guidelines
state: “The evidence justifies… the reduction of
calories from fat… to 30 percent, calories from saturated fat to 10 percent or
less, and dietary cholesterol to no more than 250 or 300 mg daily.” But
in Lipids 2010 in
a thorough review article on dietary intervention: “Diets
appear to have beneficial lipoprotein effects in individuals with atherogenic
dyslipidemia, compared to high-carbohydrate diets; whereas the content of total
fat or saturated fat in the diet appears to have little effect.” Given the diet-fat-cholesterol myth, doesn’t
entail that all diet are junk. So what
diets are beneficial?
The
short answer is those that lower oxidative damage. The main cause lies with
carbohydrates that produce
significant amounts of reactive chemicals that can oxidize small dense type-B LDL.
The process centers around glycation, ”which is the result of typically covalent bonding
of a protein or lipid molecule with a sugar molecule,
such as fructose or glucose,
without the controlling action of an enzyme.
All blood sugars
are
reducing molecules.
Endogenous glycations
occur mainly in the bloodstream to a small proportion of the absorbed simple
sugars: glucose, fructose,
and galactose.
It
appears that fructose and galactose have
approximately ten times the glycation activity of glucose, the primary body
fuel.[6] Some glycations are benign, but others are
more reactive than the
sugars they are derived from, and are implicated in many age-related chronic
diseases such as cardiovascular diseases (the endothelium, fibrinogen, and collagen
are damaged), Alzheimer's disease (amyloid proteins
are side-products of the
reactions progressing to AGEs),[7][8]
cancer (acrylamide and
other side-products are
released), peripheral
neuropathy
(the
myelin is attacked), and other sensory
losses such as deafness (due to demyelination). This range of diseases is the result of the
very basic level at which glycations
interfere with molecular and cellular functioning throughout the body and
the release of highly oxidizing side-products such as hydrogen peroxide. Long-lived cells (such as nerves and different types of brain
cell), long-lasting proteins (such as crystallins of the lens and cornea), and DNA may
accumulate substantial damage over time. Cells such as the retina cells in the eyes, and beta
cells (insulin-producing) in the pancreas
are
also at high risk of damage. Damage by glycation results in stiffening of the
collagen in the blood vessel walls, leading to high blood pressure, especially
in diabetes.[9] Glycations also cause weakening of
the
collagen in the blood vessel walls which may lead to micro- or macro-aneurisms;
this may cause strokes if in the brain” Wiki. (Note that glycation is unrelated to glycemic
index, insulin index and glycemic load.[10]) Pharma
always makes marketing decisions and thus is not motivated to prevent AS, and
will oppose prevention
through their marketing science. Thus pharma
as teacher ignores the main culprit: oxidative
damage mostly through the process of glycation to type B (small hard) LDL[11]. Pharma followed its pattern of selling the
disease and then selling the treatments.
Having sold us on cholesterol-CVD
link, they sell us the fix. So are their
drugs effective for preventing acute ischemic events?
[1]
It has been noted that with hypertension there is a response in the endothelium
cells that accelerates the thickening of the artery wall in response to the
increased blood pressure (see). But that increase is blood pressure is
initiated by AS in over 90% of cases.
A few cases of HT are associated with genetic s, drugs, and extreme prolonged
emotional
stress which produces an excess of certain neurotransmitters. Supposedly in
such cases there would be
prolonged HT but a thickening of the
wall but minimal plaque; however, I could not find definitive autopsy study of
such patients.
[2] There is an increased risk of blood clotting
with hypertension that contributes to the occlusion of the coronary artery
plugged by the leaked soft plaque. HT
is not essential for those with
normal blood pressure who have an ischemic event also benefit, when
administered early, from thrombolysis (clout busting drugs). drugs used
to ting this hypothesis of higher
incidence of clotting is sketchy.
[3] The most significant free radicals are
the
products of metabolism and carbon monoxide which results from incomplete
combustion such as from fires including cigarette smoke. Pack-a-day smokers
double their risk of death
from MI.
[4]
Downplaying infective cause entails not promoting testing long-term CPR.
Since CPR is elevated during
an infection, a short-term elevation is misleading, because AS develops over
decades. Women under the age of 55 are protected by
estrogen, thus including them in a study is also misleading are doing
short-term CPR testing are two ways for pharma to tweak results as desired.
[5]
In the 80s extensive research was done looking estrogen type protection from CVD
for men. None were marketed because these analogues
blocked testosterone, and thus caused ED and loss of strength. Today prevention
doesn’t fit pharma’s
business model.
[7] There are other causes, nothing is
simple: “Resistin, a protein secreted by
fat tissue, has been shown to increase the
production of LDL in human liver cells and also degrades LDL receptors in the liver” Wiki.
[8]
Jonny Bowden . Ph.D. & Stephen Sinatra,
MD, The Great Cholesterol Myth: Why Lowering Your Cholesterol Won’t Prevent
Heart Disease—and the Statin-Free Plan That Will, Fair Winds Press,
Nov. 2012; a national bestseller, has 23
experts who praised the book and are quoted on the cover & first page,
and at Amazon has a 4.8 star rating from
220 reviewers. Getting a fair review of
book is iffy because of heated nature of the topic and many the subscribers to
pharma’s spin. JK finds the book well
supported in the critical portions on cholesterol’s role; but in spots
questionable as to the alternative approaches to prevention of CVD.
A couple of years before reading this book, JK had arrived at those same
conclusion as to risk of CVD and on
some of their fixes.
[9] “Atheroma is
an accumulation and swelling in artery walls made up of
(mostly) macrophage cells, or debris, and
containing lipids (cholesterol and fatty acids), calcium and
a variable amount
of fibrous connective tissue… in the early stage an
accumulation of mostly macrophages, that have taken up oxidized LKL” Wiki.
[10] “Glycemic Index
(GI): A measure of the blood-glucose
level over 2 hour after 12 hours of fasting to a certain quantity of food,
usually 50 grams based on the measurement of 10 subjects. High GI is associated
with an increase in glycation, the process of
forming a covalent bond of a protein or lipid molecule with a sugar molecule,
of which some of these molecules release
highly oxidizing side-products such as hydrogen peroxide. Thus glycation
and GI are associated with an
assortment of conditions including CVD, cancer Alzheimer’s diseases, peripheral
neuropathy, sensory loss, diabetes and obesity. A more accurate measurement
than GI would be
that of the amount of glycation or the insulin level (insulin index) which is
determined by blood-sugar level. Some of
the GI figures do not accurately reflect the insulin response. Even better would
be a measurement of the
amount of the glycation CVD, cancer Alzheimer’s diseases, peripheral
neuropathy, sensory loss, diabetes and obesity. A more accurate measurement
than GI would be
that of the amount of glycation or the insulin level (insulin index) which is
determined by blood-sugar level. Some of
the GI figures do not accurately reflect the insulin response. Even better would
be a measurement of the
amount of the glycation of protein and lipoproteins” Wiki and Wiki.
[11] There are other ways glycation contributes
to
AS:
“Advanced glycation end products (RAGE)…. Soluble AGEs activate monocytes [become macrophages after entering tissue],
and AGEs in the basement membrane inhibit monocyte migration. AGE-bound RAGE
increases endothelial permeability to macromolecules. AGEs block nitric oxide
activity in the endothelium and cause the production of reactive oxygen species”
Advanced Glycation
End Products, 2006.
Statins lower TC about 30%, but
they have nearly no effect on
ischemic events. This is the conclusion
I drew from Braunwald[1]
on statin for the prevention of major events.
An article in Therapeutics letter
came to the same conclusion doing a meta-analysis using some of the same major
clinical trials: “This cardiovascular benefit is not reflected in 2 measures of
overall health impact, total mortality and total serious adverse events.
Therefore,
statins have not been shown to provide an overall health benefit in primary
prevention trials.” And repeated in JAMA
in a meta-analysis of 11 studies that included the clearly cooked Jupiter and
TNT Studies[2]. Assuming for good reason there
was major positive bias, which is the industry norm; the
actual results are significantly negative. A reasonable conclusion is that there
is
moderate benefit for some of those in the highest risk
group: unstable angina, diabetes,
previous heart attack, TC above 350, and current
smoker. No more than 5% of all those
taking statins would have a net benefit.
And if they choice lifestyle
changes, they all would benefit more than from a statin. Given the affects of
statins and hypertensive
drugs on muscle strength and cognitive function, the probability of lifestyle
changes is very significantly reduced. Taking
a statin has a significant negative effect upon quality of life, especially
among those above the age of 60. Sexual
dysfunction, reduction in strength, and decline in cognitive functions has not
been measured in pharma funded and government trials. However in the vast body
research and
clinical trial on statins, the negative consequences are exposed. In my article
on statins fourteen of them were listed:
14 NEGATIVE EFFECTS: One,
ED, it lowers
testosterone , and nitrous
oxide thus causes
ED;
a similar effect upon women for the sex steroids are synthesized from cholesterol.
Two,
COX-2
inhibitor, just like Vioxx: Vioxx
given to elderly increased heart
attacks (MIs) over 300%[3]. The American Heart
Association warns:
“accumulated
evidence that non-steroidal, anti-inflammatory
drugs [NSAIDs are COX inhibitors], with the exception of aspirin, increase risk
for heart attack and stroke.” They promote
atherogenesis. Three, blocks production of Q10, which enters
LDL and inhibits oxidative
damage that causes atherogenesis, and. Four, plaque instability: “Vulnerability of
plaques to rupture and thrombosis is of greater clinical
relevance than the degree of stenosis they cause” (Corti et al., 2003). “Statins affect plaque stability in
a variety of ways. The meta-loproteinases degrade extra-cellular matrix components and thus “weaken
the fibrous cap and destabilize the
lesions” -- Goodman and Gilman pharmacology, 11th Ed, p
950. Rupture of plaque causes over
80% of MIs. Statins inhibit secretion
MMP-1, 3, & 9 from SMC, and microphages make plaque less stable. Five, reduction
in ATP: Q10 (CoQ10) is needed for
the conversion of APD to ATP (adenosine-5-triphosphate),
the source of energy for muscles contraction.
“ATP is often called the ‘molecular unit of currency’ of intracellular energy transfer including muscle contraction and for
chemical reactions. ATP transports
chemical energy within cells
for metabolism”--Wikipedia. A reduction of
40% in CoQ10 is accepted.[4]
Six,
The heart muscle under stress needs more ATP, not less. This is why pharma excludes
the elderly and
those with coronary heart failure (CHF)
from trials. “This may explain
previous reports that the mean age of ME/CFS patients
dying from CHF are 2.5 years younger
than the control group.” In a
summary of journal articles which concludes:
“As the potency of statin drugs increases and as the target LDL
cholesterol level decreases, the severity of Q10 depletion increases and
heart-muscle function declines. This tragic
scenario may very well be prevented by using supplemental Q10 with all HMG
CoA reductase inhibitors [statins]” and, and. Thus “Lower cholesterol, poorer
outcome
in CHF patients.” Pharma ignores Q10 side effect. Seven, All Statins
inhibit the rate controlling enzyme HMGCR of the mevalonate pathway. “This
pathway
generates a range of other products in
addition to cholesterol, including coenzyme Q10, heme-A, the production of dimethylallyl prophosphate (DMAP), and isopentenyl pyrophosphate(IPP), which serve
as the basis for the biosynthesis of molecules used in processes as diverse as
terpenoid synthesis, protein prenylation and isoprenylated
proteins10 which have pivotal roles in cell biology and
human physiology and potential relevance to benefits as well as risks of
statins.11-13 Drugs, such as the statins, stop the
production of mevalonate by inhibiting HMG-CoA reductase”.[1]
Wiki “The Mevalonate pathway is important
for, cell membrane
maintenance, hormones, protein anchoring, and N-glycosylation. It is also a part of steroid biosynthesis” (Wiki). “Dolichols
are isoprenoids synthesized from mevalonate. They are vital to
the process of Glycoprotein formation in the endoplasmic reticulum of cells. In this capacity it is critical to the
formation of the Glycoproteins involved in neuro-peptides, cell
identification, cell messaging and Immune defense. Reduced bioavailability of dolichols can affect every cellular process in
the body” Wiki. And this
is only a partial list. Eight, Cholesterol
is essential for life. “It is the precursor
for the biosynthesis of steroid hormones, bile acids, vitamin D, and is an essential component of cell membranes
for
proper permeability and fluidity. Effects
include
pancreatic and hepatic dysfunction, ED, diabetes[5],
muscle weakness and myopathy (muscle disease). The myelin is a cholesterol base
coating around nerve cells[6]
(Wiki). Nine, Cognitive: the reduction Q10 & cholesterol for the myelin
sheath causes cognitive decline--especially in the elderly where it often
leads to an incorrect diagnosis of Alzheimer’s disease and to neuropathy. Ten, Side
effects account for the poor compliance in the elderly (25%
use at 2 years).
Poor
compliance also occurs with
elite athletes. Eleven, Fails to
reduce ischemic events because atherosclerosis is caused by oxidative damage to LDL,
not high levels of LDL; thus statins are ineffective. Three out of 4 major studies
of secondary prevention
(ALL-HAT, ASCOT, & PROSPER) failed
to find life extension from statins (Table 42-78, Braunwald’s Supra,
p 1085).
This table stands in opposition to the “safe & effective”
claim (p 2286), which is pharma’s mantra, a mantra supported by their marketing
studies and guidelines. Junk
science is the norm on TNT
trial (p 3). Thirteen: For high risk primary “no
benefit on all-causes of mortality”. [7]
Fourteen,
women in those 4 major studies showed less
benefits then men treated with statins; they have less AS because of estrogen.[8] Thirteen,
Drug interaction with serious side effects are common (and under reported). The system for reporting barely
functions.
The results
for statins are dismal:
“A
meta-analysis of predominantly industry sponsored data reported that in a low
risk group of people aged 60-70 years taking statins the number needed to treat
(NNT) to prevent one cardiovascular
event in one year was 345. … In this
group [patients who had suffered an MI] the NNT is 415 for mortality over one
years. This doesn’t mean that each patient benefits a little but rather that
414 will receive no prognostic benefit.”
So, why do doctors have faith in statins? As stated on page
2, the 800 pound gorilla has replaced evidence based medicine with expert based
medicine, and the gorilla owns the clinical trials and provides the thought
leaders. These thought leaders repeat
the mantra “safe and effective” which is also repeated in cardiology textbooks
and guidelines. Secondly the thought leaders teach that plaque formation is
strongly correlated with the TC and
LDL blood levels, and thus the 30% average reduction in TC is assumed to entail
a corresponding reduction in ischemic
events, which is confirmed by their best marketing studies, which minimalizes
side effects, of course. All this is fed
to physicians in continuing education classes given to promote drugs. All patented
drugs are improvement that are
safe and effective. Peer-pressure and
the need to follow guidelines play an important role in marketing statins and
promoting the cholesterol myth.
So why
does the FDA allow this to go on unchecked.
As stated on page 2, the FDA functions as an extension of pharma. This
failure to supervise in the public’s
interest is not a topic for corporate media; but it is published
elsewhere. See for example the article Consumer
Report article FDA: From Watchdog to Lapdog? Prof Marcia Angell in her book The
Truth About the Drug Companies, chapter 12, gives a detailed history of
how Congress was
persuaded to pass pharma-friendly legislation.
Today it is the norm for pharma to find a select group who benefit from
a drug and then expand its usage to a much larger population. Merck tested Mevacor
(the first statin) on a
very select population of those with familial hypercholesterolemia (FH,
about 1 in 1,500). They
have a genetic defect which causes their cholesterol to be several times above
the norm.[9] The surrogate end point lowering TC was used for FDA approval. Moreover, “there
are no interventional studies that directly show mortality benefit of
cholesterol lowering in familial hypercholesterolemia patients” Wiki, That is why Merck for Mevicor’s
used
the surrogate endpoint lower TC. Once
approved, their marketing department went
to work. Now pharma, based on
AstraZeneca’s Jupiter Study, has lowered the guideline bar: “US
recommendations for
low density lipoprotein cholesterol concentrations could put most of
the Western world's adult population on statins. This is the message from the American National Cholesterol Education Program published
last
year.1… Recently,
Getz et al calculated that in Norway, one of the healthiest nations in the
world, about 85% of men and more than 20% of the women over age 40 would be
classified as high risk using this criterion.”2 The
BMJ article then listed the known
side effects of statins, quite different than the safe sales mantra. But our
physicians won’t hear of side effects
in pharma’s continuing education classes, nor will the public from our
corporate media. “The government’s
obsession with levels
of total cholesterol, which has led to the overmedication of hundreds
of millions of people with statins, has diverted our attention from the more
egregious risk factor of atherogenic dyslipidaemia” BMJ.
Since statins
though they lower TC, they don’t prevent endpoint events,
and diets doing the same also fail, what should be done to reduce risk? There
are life-style changes and drugs that
reduce the causes for oxidative damage to LDL and others the inflammation
response. It is rather a tricky proposition to long-term reduce the immune
response with a drug can increase the risk for chronic and acute diseases. The
immune system fights off pathogens and promotes the death of abnormal cells including
in tumors. The other path is to lower oxidative damage, and this is a win-win
situation in that there are other benefits including protection of the
mitochondria. Life style changes are
equally important because they reduce oxidative damage.
Lifestyle
makes a difference. The greatest gains are from weight control, low-carbohydrate
diet, cessation of smoking, and vigorous exercise. Rapping the heart in
a layer of fat and
making the heart pump harder through miles of blood vessels are consequences of
obesity. Moreover with obesity, fat
adversely affects the feedback mechanism that regulates insulin; thus the risk
of type-2 diabetes increases 30 fold.
Diabetes causes a higher level of blood borne sugars thus increases the amount
of glycation. Diabetes causes red blood
cells to leak out of capillaries which cause an immune response by
macrophages. For these reasons diabetes doubles
the rate of MI. Diabetes shortens
life an average of 5 years
and with obesity more. Carbon
monoxide--a reactive chemical that damages LDL-- from tobacco doubles the rate MI.
A pack-a-day smoker shortens their life on an
average 7-12 years. Carbon monoxide
promotes the production of unstable plaque, thus with cessation, the risk for MI
dramatically drops over the next 5
years. Vigorous exercise strengthens the heart, improve
vascularization, an anti-inflammatory, and healthful effects upon the epithelium cell (walls)
of arties. Controlling for lifestyle
contravening variables, senior runners extended life 8.7 years, & it improves
quality. “Exercise capacity is a
powerful predictor of mortality” NEJM.
Diet makes a difference, but not the diet that pharma & our government teach which
promote the fat-cholesterol myth. In 11
out of 12 studies reviewed in Wikipedia, results did not have a benefit from low
fat, or increased ratio
of polyunsaturated fats “A meta-analysis of 21 studies considered the
effects of saturated fat intake and found that Intake of saturated fat was not
associated with an increased risk of CHD (coronary heart disease), stroke, or
CVD (cardiovascular disease)"[7]
Wiki.
The
main diet culprit in
CVD is glycation of proteins and lipoproteins which produces reactive
chemicals that cause oxidative damage to proteins and lipoproteins. One source
of reactive chemicals comes from
the glycation of LDL. A high sugar diet (especially
fructose) is associated with insulin resistance, diabetes, and metabolic
syndrome; all are causal factors for AS.
Fat as stated before is not the culprit:
“Indeed, recent prospective cohort studies have not supported any
significant association between saturated fat intake and cardiovascular risk.5 Instead,
saturated fat has been found
to be protective. The source of the saturated fat may
be important. Dairy foods are exemplary providers of vitamins A and D. As well
as a link between vitamin D deficiency
and a significantly increased risk of cardiovascular mortality, calcium and
phosphorus found commonly in dairy foods may have antihypertensive effects that
may contribute to inverse associations with cardiovascular risk.6 7 8 One study showed that higher concentrations of plasma
trans-palmitoleic
acid, a fatty acid mainly found in dairy foods, was associated with higher
concentrations of high density lipoprotein, lower concentrations of
triglycerides and C reactive protein, reduced insulin resistance, and a lower
incidence of diabetes in adults.9 Red meat is another major source of saturated fat.
Consumption of processed meats, but not red
meat, has been associated with coronary heart disease and diabetes mellitus,
which may be explained by nitrates and
sodium as preservatives.10
… Adopting a Mediterranean diet after a
heart attack is almost three times as powerful in reducing mortality as taking
a statin.
The recently
published PREDIMED randomised controlled trial was stopped early after it
showed that in high risk people the Mediterranean diet achieved a 30%
improvement over a “low fat” diet in terms of cardiovascular events”22 BMJ. A low-fat,
high carbohydrate diet increases
the intake of foods with sucrose and high fructose corn sweeteners, and fruits
also a source of fructose. The
Mediterranean diet is also low sugar. They
promote glycation of fructose driven oxidative damage to LDL[10].
“Glucose is the primary
food source of energy for the body cells—with a few exceptions. Glucose is transported
from the intestines or liver to body cells via the
bloodstream, and is made available for cell absorption via the hormone insulin,
produced by the body primarily in the pancreas. The
body's homeostatic mechanism keeps blood
glucose levels within a narrow range. It
is composed of several interacting systems, of which hormone regulation is the
most important. Insulin decreases
blood glucose. If blood sugar levels
remain too high the body suppresses appetite over the short term. Long-term hyperglycemia causes many health
problems including heart disease, eye, kidney, and nerve damage” Wiki. A second health consequence is from glycation
(as prior discussed). Glucose, a monosaccharide, has
1/10th the glycation
potential of fructose; and glycation
results in oxidative damage in the body including to LDL the main cause for AS.
Fructose is found in many plants, especially
the fruits. Sucrose (commercially from cane
and beet sugar) is a disaccharide consisting of glucose and fructose. Glucose
has 1/10th the glycation rate of sucrose. Note high fructose corn syrup (HFCS) is 24% water; the rest
is
glucose-fructose with a moderately elevated level of fructose (approximately
55% and glucose 42%). Thus though 31%
higher in fructose (13/42) than sucrose (50-50 of each) because it glycation
rate is 10 fold that of glucose, there is 300% more glycation. (Note glycemic index and glycemic load are not
measurements of glycation, but measurements of blood serum glucose after eating
a quantity of food.) Though claims are
made that HFCS is statistically linked
to diabetes, obesity, and metabolic syndrome, the laboratory evidence is thin,
and diverts attention from its link to oxidative damage of LDL and AS.
Carbohydrates are needed for the
glucose that drives the ATP production (energy) and to be stored as a reserve
as glycogen in animals. Fructose is also metabolized in a process leading to the
synthesis of glycogen, and fructose at this point is also used for the production
of fatty acids and triglycerides. The
best of carbohydrates are starches since they lack fructose and thus are less
subject to glycation than sucrose and fructose.
Most starches are very long chain of glucose molecules most of which are
in subunits, the water soluble amylose and insoluble amylopectin. Starches are
the best source of glucose, while
sucrose and HFCS the worse.[11] The
best are starches, the worse are foods high in fructose and galactose (one half
of the disaccharide lactose found in
dairy products of which milk is by far the main source.)
Since those
living in Mediterranean
countries have a significantly lower rate of CVD, and genetics is not the
reason, it is assumed that diet is the reason. Sorting out what works in a Mediterranean diet requires laboratory
experiments. First the fat-cholesterol
myth entails that the praise of polyunsaturated fats misses the mark. First
“olive oil consumption is negligible…”moreover, Mediterranean countries tend to consume relatively high
amounts of fat, they have far lower rates of cardiovascular disease than in
countries like the United States, where similar levels
of fat consumption are found. The
inclusion of red wine is considered a factor contributing to health as it
contains flavonoids with powerful antioxidant properties. A
healthy lifestyle (notably a physically active lifestyle or labour) is also
beneficial… The proposed mechanism is solar UVB-induced synthesis [sun] of
Vitamin D in the oils of the skin, which has been observed to reduce the
incidence of coronary heart disease, and which rapidly diminishes with
increasing latitude. Mediterranean, low-sugar,
low-glycemic index, and high-protein diets are effective in improving markers
of risk for cardiovascular disease and diabetes. A recent randomized Spanish
trial of diet pattern published in The New England
Journal of Medicine in 2013 followed almost 7,500 individuals
over around 5 years found that individuals on a Mediterranean diet supplemented
with mixed nuts and olive oil had a 30 percent reduction in risk of having a major
cardiovascular event and a 49 percent decrease in stroke risk” Wiki. In summary antioxidants in red wine and dairy
products with vitamin D and increased exposure to sun light, the low glycemic
index of diet, & low fructose[12] all have positive
effects. The details from the lab uncovered
what in their diet works. In addition
the lack of sedentary lifestyle, especially the elderly, and walking in hilly
areas further significantly contribute.
Three
very effective drugs: each has a proven
track
record; and they have additional health benefits besides significantly lowering
the risk of CVD. Pharma has done
mountains of marketing
studies to sell hypercholesterolemia and the use of statins. Similarly pharma
has done studies to dissuade
doctors and public from the usage estrogen and aspirin by claiming their benefits aren’t
worth the risks. See Aspirin and Natural HRT for an exposure of the junk science
on risks; and also for a list of their many benefits. Since there are
no side effects from Q10, pharma ignores Q10 and does junk
science to deny its benefits. These
drugs effectiveness is more proof as to the role of oxidative damage to LDL and
the immune response, and they significantly reduce the risk of other major
conditions.
As stated
above there are risk
associated with immunosuppressant drugs.
The most popular are the NSAIDs (non-steroidal anti-inflammatory drugs)
all increase very significantly the risk for ischemic events through their
inhibition of the COX-2 (Cyclooxygenase)
a prostaglandin hormone, but for aspirin[13]. In a news release:
“Many
doctors should
change the way they prescribe pain relievers for chronic pain in patients with
or at risk for heart disease based on accumulated
evidence that nonsteroidal anti-inflammatory drugs (NSAIDs), with the exception
of aspirin, increase risk for heart attack and stroke”, advice issued by the American
Heart Association.. Vioxx and several
others have been pulled from
the market for this reason. Long-term Vioxx use
increased the risk of MI over 300%,
and naproxen (Alive) by at least 50%.
This has been known for a decade, yet NSAIDs are taken long-term by
millions for joint pain and arthritis.
Aspirin: In the 1950s, when I was growing up,
aspirin was the dominant over-the-counter drug for mild pain, arthritis,
anti-inflammatory, and colds. It came in
500 mgs, and the initial dose was 2, followed by 1 every 3 hours, or as
needed. The standard daily usage for
arthritic and joint pain, and chronic lower back pain was 2.5 grams per day,
with 7.5 grams as the upper limit—this continued to be recommended by doctors
until the 1990s. Annual production
reached a peak in the U.S. of 20,000 tons in 1958. Nothing has changes since
the 1960s as to its
risk factors; and several major benefits were since discovered including those
of prevention of blood clots, heart attacks, cancer,
atherosclerosis, Alzheimer’s, and
increased cancer survival, yet its sales have decline until now it is 8th. Most
sales are for the ineffective under 100
mg dose for those at risk of a heart attack—tolerance develops to the
antiplatelet effect within 1 year.
Aspirin is the only safe NSAID.
The American Heart Association warns that all NSAIDs[14]
increase significantly the risk of heart attack but for aspirin[15]. Being 8th
is proof that pharma
controls drug usage. Among its
significant benefits are prevention of hardening of the arteries,
cancer, Alzheimer’s disease, and thrombosis which causes heart attacks,
strokes, pulmonary embolism, and kidney damage.
Aspirin reduces significantly the top three killers. Because of its anti-inflammatory
action, “It
is the standard against which all rheumatoid arthritis medication should be
measured” Goodman & Gilman 11th Ed, 2006. Aspirin is
the drug of choice for
osteoarthritis, Merck Manuel 15th Ed. p 973. Aspirin’s anti-inflammatory
action prevents hardening
of the arteries, which is essentially an inflammatory process that oxidizes LDL.
Aspirin stimulates the body’s mechanism for destruction of abnormal
cells (necrosis factor) including trauma damaged cells and precancerous and
cancerous cells. By doing so it both
prevents most cancers and promotes survival.
For example, with breast cancer the rate is reduced over 40% and
survival of stages I, II & III is increased over 60% (doesn’t affect
metastatic cancers). Yet the FDA gives
it the lowest approval rating for cancer treatment. Pharma attacks the usage
aspirin because it
would drastically reduce the sales of nearly half their blockbusters. Besides
ignoring aspirin’s benefits, pharma
has blown out of proportion its health risks.
Doctors automatically blame aspirin for all major & minor bleeding
episodes, though scientific studies shown an increases the risk of ulcer 4%
over 5 years. This occurs because of pylori bacteria in their stomach that has
penetrated the protective mucus membrane.
Goodman and Gilman supra, comment that “many clinicians favor the use of
other NSAIDs perceived to have better gastrointestinal tolerability, even
though this perception remains unproven by convincing clinical trial”.
And to prevent the next generation from
taking aspirin, pharma and the FDA warn about Reyes Syndrome. Once diagnosed
based on symptom with 555
cases in 1980; now with the advent of genetic testing for the metabolic
syndrome it dropped to two cases in 1994.
This drop in frequency is ignored by pharma and the FDA. Finally on dosage: pharma reduced aspirin from 500 to 325 mg,
and initial dose from 1 gram to 325 mg, which is too low to be effective for
pain and inflammation. Effective dose
for pain and arthritis is 2.5 g m daily.
For prevention of blood clot (thrombosis) cancer, atherosclerosis, and
Alzheimer’s disease 325 mg once or twice daily, and twice that amount as
chemotherapy for cancer. For over 50
years 2.5 grams or more taken by millions for arthritis--the 1987 Merck Manual
recommends 3.5 grams daily. The
increased ulcer risk was known for over a century, but it took pharma’s
unwarranted assault to change doctor’s opinion.
Moreover the other
NSAIDs increase the risk of ischemic heart attacks and strokes, and acetaminophen (Tylenol) causes triples
the risk of asthma in children and is the leading cause of drug induced liver
failure. Tens of millions have died
early from cancer, ischemic heart attacks & strokes, and Alzheimer’s
disease because the marketplace has no conscience.
Q10 (CoQ10): recognized as the most effective antioxidant.[16]
A number of major health conditions
are caused by oxidative damage including hardening of the arteries for which
Q10 is protective. Q10 is found in every cell in the body because
it is used by the mitochondria in the production of ATP from glucose. ATP accounts
for 95% of the body’s
energy. The
antioxidant effect of Q10
derives from its energy carrier function
in the production of ATP. As an energy carrier, the Q10 molecule
is continually going through an oxidation-reduction cycle. It is the best of anti-oxidants because it is
distributed throughout the body, in every cell.
It is found in LDL and thus protects by preventing oxidative damage to
LDL which is the initial step in the
process that result in AS & CVD.
It protects other tissues from oxidative damage and thereby reduces the
risk for a number of serious conditions including Alzheimer’s & Parkinson’s
diseases, CVD, and macular
degeneration. The second important
function is protection of the mitochondria
from damage from the reactive chemicals produced in the metabolism of
glucose. Decline in endurance & peak
performance with age is a result of oxidative damage to the mitochondria for
which Q10 slows that process. It is
particular beneficial for those with heart disease, hypertensions, diabetics;
and for those taking statins or beta blockers (for hypertension) for these
drugs partially block the bodily production of Q10 (40% for statins) and the
other products of the mevalonate pathway.
All these benefits from long-term Q10 add up to an increase in lifespan
and greater endurance. Q10 is not
toxic: a study found that daily dose of
3600 mg was well tolerated by both the healthy and unhealthy patients. Recommendation: 100 mg for children, being gradually
increased to 300 mg by the age of 40--and its yearly cost through Costco is
under $70 for Kirkland brand Q10.
Natural Estrogen (Estradiol) with
progesterone HRT: What every woman should be taking because of
the numerous, major health benefits, benefits that would slash pharma’s
profits. As Dr. Ben Goldacre says, “the
devil is in the details.” Of the 4
natural estrogens, only estradiol (E2,
17β-estradiol) has major benefits. Two (estriol (E3) and estetrol (E4)) are found in pregnant women.
They should not be used in HRT because they
block estradiol’s action. Big pharma
being against hormone replacement therapy (HRT) markets ineffective products at
too low a dose, and Prempro, the most popular HRT is the worse. Based on marketing
science, including the
major WHI clinical trial by the FDA
which knowingly used Prempro, a combination of estrogen derived from pregnant
mare’s urine and the progestin MPA. The
biological effects of mare’s estrogens are different than human estrogen and
MPA blocks most major of the benefits of estrogen. Because of the use of Prempro
the result of
the WHI contradict other
trials. The finding for Prempro[17] cannot be validly applied to the natural
estradiol and progesterone—though pharma and the FDA did. The FDA warns
that hormone replacement
therapy has only one valid medical use, to manage hot flashes, and it should be
used at the lowest dose for the shortest time.
Earlier trials and epidemiological studies found that HRT lowers Alzheimer’s 83%, heart attacks 32%, coronary
heart disease 50%, colorectal cancer 46%, breast cancer 73%, thrombosis 8%,
osteoporosis fractures 90%, macular degeneration 65%, reduces & prevents
arthritic join destruction, firmer breasts, healthier skin
(less wrinkles, thicker, 48% more collagen), reduces hair loss, improved
cognitive function, less depression and mental illness, and a general feeling
of well-being with increased libido. Estradiol
is the most effective treatment to prevent osteoporosis—bisphosphonates the
worse. Estradiol’s methods of
cardiovascular protection are well documented.
The lack of estradiol is the
reason for the precipitous decline in health of women. The brouhaha over
estrogen receptors and
breast cancer is based on marketing science.
Life extension with long-term natural HRT is at least 4 years. Because
of an
increase in a low incident cancer (uterine), a progestin (synthetic
orally active hormone with some progesterone properties) is added to hormone
replacement therapy rather than the natural progesterone which isn’t orally
active—except when micronized and suspended in oil. The best method of
application is a lotion
obtained from a compounding pharmacy in a dose of 4 mgs estradiol plus 100 mg
of progesterone per application--absorption
rate is about 15%. Apply widely
as possible over the torso, back, shoulders, underarms, and face using
water and rubbing it in to promote better absorption. Recently progesterone has been micronized in oil and
available as a pill. Ideal free-serum estradiol level is 7-9 pg/mL. A compounding pharmacy can prepare a pill consisting of 2 mg
of estradiol with 50 mg of progesterone.
The lotion form is better for the skin.
Plant sources of estrogens are not very effective. Doctors who follow
the Wiley Protocol are
other methods of hormone balancing for post-menopausal women are milking the
insurance and patient, it lacks sound scientific evidence. Keep it simple.
Testosterone: the
male hormone that is almost identical in structure to estrogen and thus has
many of the same benefits as estrogen.
Noticeable benefits for testosterone:
quality of life
in 4 weeks, depressed mood in 30 weeks, bone
mass in 26 weeks, lipid profile in 52,
inflammation in 12 weeks, sexual interest in 6 weeks, erection/ejaculation in
26 weeks, red cells in 52 weeks,
insulin sensitivity in 52 weeks ,
muscle strength in 16 weeks, fat mass in 16 weeks (Eur J Endocrinol. 2011, Nov. 675-85). Other
benefits include improved cognitive
function, reduced risk for Alzheimer’s disease, metabolic syndrome, diabetes,
cardiovascular disease and the fatal resultant heart attacks and strokes. The
brouhaha to CVD and prostate cancer are
based on pharma’s marketing science. “Testosterone does not cause or produce
deleterious effects on prostate cancer” Wiki. Recommended: once serum testosterone level
drops below 350, to use 100 mg of testosterone in a topical cream. Ideal
level in the 850 to 1200 ng/dL or
higher. Increased to 150 mg at age 75
as effects diminish--bio-receptors and response decreases with age as does the
level of free (available) testosterone.
Current assay methods are inaccurate as to
measurement
of free testosterone. Best source for
testosterone is from a compounding pharmacy.
Apply
widely
as possible over the torso, back, shoulders, underarms, and face using
water and rubbing it in to promote better absorption. Doctors who follow
a program of hormone balance are milking the insurance and patient. There is
probably a value to taking also HGH,
though how much lacks quality evidence.
|
There is a large body of clinical
trials and epidemiological studies that have shown that cholesterol and high
fat diet have minimal effect upon promotion of CVD, and conversely that a low
fat & low cholesterol diet is not cardiovascular protective (see Cholesterol Myth). As stated prior oxidative damage to LDL and
the immune response is the primary cause (infectious agents are second main
cause), thus drugs listed below have modest effect while statins for an
assortment of reasons are not worth taking (see statins). Since so many believe
in the cholesterol
myth, the natural, safer method of lowering blood cholesterol of niacin and
its inositol form are included below.
|
Niacin
family and other
natural cholesterol lowering drugs and cardiovascular disease (CVD): Some of you will as a matter of insurance
want
to lower your TC a natural way or
are taking a statin (a mistake). Pharma
recommends 1,500 to 3000 mgs of
niacin (nicotinic acid) taken with meal; however
insulin blocks its cholesterol lowering affect. High dose causes the unpleasant
flushing and
thus low compliance. The only long-term
study (usage 6 years, followed 15 years) was of high dose niacin. It produced
a reduction in deaths from
cardiovascular disease of 11%; this compares favorable to statins once the
tobacco science trials are eliminated from consideration (see Statin, Braunwald
table). However, a study based on blood
work showed that 200 mgs at bed is just as effective, and without
flushing. In the same experiment similar
results were obtained with inositol hexanicotinate, a source of niacin. Niacin
also possesses anti-inflammatory and
antioxidant benefits, and thus inhibits atherogenesis. Phenolic substances found
in red wine are of value, so too of value is
nutritional yeast, red yeast extract,
and omega-3 fatty acids (found in
fish oil). For lowering the bad
cholesterol use 200 to 500 mgs at bedtime of either niacin or inositol
hexanicotinate. There is miniscule value
of lowering cholesterol that is below 350 (though pharma promotes statins for
those above 240). Recall that pharma has
turned cholesterol into a villain.
However, as explained the most important factor for CVD is the inflammatory
response to damaged LDL, for which aspirin
and Q10, along with estrogen for postmenopausal women offers a greater benefit
than lowering cholesterol. Testosterone once
blood level is below 350 lowers risk of MI, heart failure, and metabolic syndrome. Change in lifestyle is very effective.
Following the advice
of lifestyle change, Q10,
aspirin, estradiol, and testosterone entails that statins and niacin are of no
health value. There are other
drugs of value; however, doing more is not better, but for the sake of
completeness several have shown to be of value.
D-ribose is a building block
for ATP, L-carnitine aids in the
production of Q10 and is an effective antioxidant, and vitamin
C is
an antioxidant lowers risk for AS (not recommended for those with
hemochromatosis). Magnesium 1 gm
daily is recommended for those with the issue of
high blood pressure and a significant load of arterial calcium. Coronary artery
calcification is a major risk factor for heart disease and magnesium lowers
that load (Bowden 136). Berberine,
a Chinese herbal product has
a positive effect upon TC, reduces
superoxide levels in LPS-stimulated macrophages, and is “useful for patients
with congestive heart failure…suppresses the growth of a wide variety of tumor
cells[18]” Wiki, and it lowers
blood sugars in treating diabetes. Improves TC, etc. Glutathione is an organic chemical
found in plants and animals. “It is the major
endogenous antioxidant produced by the cells, participating directly in the neutralization
of free radicals and reactive oxygen compounds, as well as maintaining
exogenous antioxidants such as vitamins C and E in their reduced (active)
forms.[17]” Wiki. The issue as to what should be taken in
addition to those listed in the recommended section. One issue is the lack of
long-term clinical
trials, and the possibility that in combination there would be adverse
consequences. As preventative
medications, those in the recommended section are totally adequate. For those
with severe CVD these additional drugs have value, depending on condition. But asking your doctor is like asking his
thought leaders. I follow my advice,
and also consumes on his foods about 5
gm per day of nutritional yeast which I find a subtle feeling of wellness like
that of drinking green tea with a meal. The
choices go back on you. We have a long
way to go before the potential of medical
science is unleashed from its corporate master.
[1] Braunwald, Heart Disease, 8th
Ed.
P 1085 table. There of the 4 major
clinical trials, 3 of them the placebo cohort had as many major ischemic events
as those treated with statins.
[2]
For a detailed account of Pfizer’s TNT Study on how the evidence was worked to
lower guidelines for statins (Lipitor).
The Jupiter study “a major discrepancy between significant reduction of
nonfatal stroke and myocardial infarction, but no effect on mortality from
stroke and myocardial infarction… raises troubling questions concerning the
role of commercial sponsors “…. ” NIH, & Wiki.
[3]
A reasonable assessment of total early deaths from the selective COX-2
inhibitors in the US would be over 200,000; and a much greater number for the
non-selective COX inhibitors, the NSAIDs—but for aspirin. Celebrex is
still on the market, and though
warnings about all COX inhibitors warning
that they promote CVD, the oft-heard
sales message prevails.
[4] After 3
months treatment of healthy patients with a poor TC using pravastatin or simvastatin, the total
cholesterol and CoQ10 (Q10) were lowered 40%, when
compared to the placebo group. “A
diminution of Q10 availability may be the cause of membrane alteration with
consequent cellular damage”—Journal
of clinical Pharmacology. This finding is
supported in other studies and widely accepted—summary article.
[5]
9% increase in risk of developing diabetes over 4 years, meta study Lancet 2010
based on pharma trials--undoubtedly under-reported.
[6]
The 2nd cause for neuropathy, the
first low Q10. The two are additive.
[7] JAMA 2010: “ In conclusion, based on
aggregate data on 65 229 men and women from 11 studies, yielding
approximately 244 000 person-years of follow-up and 2793 deaths, we
observed that statin therapy for an average period of 3.7 years had no benefit
on all-cause mortality in a high-risk primary prevention population.” And
this analysis included the low quality
Jupiter Study.
[8] Jonny Bowden & Stephen Sinatra, The
Great Cholesterol Myth, 2012, p. 124, Using several of the studies used
in Braunwald’s table (supra 1085), they found only 28% in the trial were women,
and they didn’t benefit from statins.
Pulling the 5 studies and including men, “total mortality is not reduced
by statin therapy” (at 124).
[9]
At that abnormal level the rate of oxidative damage to LDL out-paces the
cleanup process, and typically their first MI occurs in the 4 decades. But this
doesn’t prove that without other
risk factors those with a TC near
350 are at significantly greater risk.
[10] This is an example of the need for laboratory
experiments to provide the modus operandi for the results of a clinical
trial. In this case carbohydrates are
bad only in the degree that they promote glycation, and for example glucose the
rate is 1/10 that of fructose, Wiki. The right carbohydrates are a healthful
source of energy.
[11]
Common names create confusion: corn
starch contains fructose, and corn syrup is pure (35%) glucose with water. Cellulose
is a long chain of D-glucose for
which we lack an enzyme to digest, though some bacteria can.
[12]
fructose: sodas
29 gm/can, fruit juices 26-9, fruits;
apple 25 , raisin 20, honeydew 16,
strawberry
15, plum 13-10, banana 10, orange 9, pineapple 8, grapefruit 8, peach 8,
nectarine 6, peach 7, apricot 4, ; vegetables
tomato 14, cucumber 13, pepper 11,
lettuce 9-5, green bean 5-2 gm, gm, squash 9-4, cabbage 8 celery 6, peppers. Squash 13-11 gm, , carrot 2, broccoli
4-2, Sweet potato 1, potato 1, spinach 1.3, beet 1.3, pea 0.4, corn 1-1/4;
grains 1/4th milk 0.04, cheese 0.07, bread 1.3, fish 0.2, nutritiondata.
[13] Aspirin is unlike the other COX inhibitors
(the NSAIDs); they increase the risk of CVD with prolonged usage as a result of
blocking the mechanism by which atherogenesis process is shut down. Thus with
use of naproxen, Celebrex, and
other NSAIDs, the rate of atherogenesis remains high once started. These drugs
in their suppression of COX-2
thereby suppress “dependent cardio-protective prostaglandins, prostacyclin in particular” Wiki. On the technical
side, it seems that Pfizer in the promotion of Celebrex has offered a clotting
mechanism for increased MI while ignoring its atherogenesis effect. Namely,
COX-2 inhibitors promote blood clots
through blocking the mechanism for breaking up blood clots through blocking the
production of prostacyclin. This explanation is contracted by the fact that incidents
of MI goes up over time for those at high risk & not low risk, nor with
short-term use. Also contra clotting
explanation is that the risk persists after stopping “in 1 year after Vioxx was
stopped there was a 75% greater risk … at.
[14] NSAID are None Steroidal Anti-Inflammatory Drug, this
includes naproxen in Aleve, ibuprofen, Celebrex, and over 30 others. Naproxen,
for example, has been shown when
taken long-term to increase the risk of heart attacks at least 50% and Celebrex
200%, yet both are widely prescribed for arthritis. Vioxx was removed by Merck
(pending FDA
actions) when it was shown to increase the death rate from heart attacks by
400% in a study on the prevention of Alzheimer’s disease.
[15] The mechanism is through an atypical
effect
of aspirin (but not other NSAIDs) through the stimulation of the production of
15-LO which is anti-inflammatory. The
other NSAIDs through promotion of 5-LO activity increase the risk of MI, as
demonstrated in a study of an Icelandic population—at AHA and.
[16] Gluathione also highly rated antioxidant,
Berberine a plant product with Lipid lowering properties, Vitamin D
administered with calcium Inositol hexaphosphate (phytic acid) has promising
claims. All these at this point have not
been sufficient reviewed for a claim to be made thereon.
[17] Prempro has been the leading selling
HRT
since the mid 40s in the US, and it still is.
The issues with MPA and mare’s urine estrogen have been know for decades
by scientist including those in the FDA, as too the superiority of the natural
HRT. Because of birth control pills,
HRT, and the possibility that an estrogen would protect men—as it does women—from
cardiovascular disease, there has been thousands of published articles on the
estrogen and progesterone family of hormones.
[18]
Berberine
has drawn extensive attention towards its antineoplastic effects.[63][64] It seems
to suppress the growth of a wide variety of tumor cells, including breast
cancer,[65] leukemia,
melanoma,[66] epidermoid
carcinoma, hepatoma, pancreatic cancer,[67] oral
carcinoma, tongue carcinoma,[68] glioblastoma,
prostate carcinoma and gastric carcinoma.[69][70] Animal
studies have shown that berberine can suppress chemical-induced carcinogenesis,
clastogenesis,[71] tumor
promotion, tumor invasion,[72][73][74][75][76] prostate
cancer,[77][78][79][80] neuroblastoma,[81][82] and leukemia.[48][83]
It is a radiosensitizer of tumor
cells, but not of normal cells. How berberine mediates these effects is not
fully understood, but its ability to inhibit angiogenesis and to modulate
Mcl-1, Bcl-xL, cyclooxygenase (COX)-2, MDR, tumor necrosis factor (TNF)- and
IL-6, iNOS, IL-12, intercellular adhesion molecule-1 and ELAM-1 expression,
MCP-1 and CINC-1, cyclin D1,[84]activator
protein (AP-1), HIF-1, PPAR-, and topoisomerase II has been shown. By using
yeast mutants, berberine was found to bind and inhibit stress-induced
mitogen-activated protein kinase kinase activation. Because apoptotic,
carcinogenic, and inflammatory effects and various gene products (such as
TNF-α, IL-6, COX-2, adhesion molecules, cyclin D1, and MDR) modulated by
berberine are regulated by the transcription factor nuclear factor- B (NF- B),
it is postulated this pathway plays a major role in the action of berberine.[85] Berberine
suppressed NF-κB activation
induced by various inflammatory agents and carcinogens. This alkaloid also
suppressed constitutive NF-κB activation found in certain tumor cells. It seems
to protect against side effects of radiation therapy in lung cancer.[86] However,
new studies suggest that while berberine decreases cell growth, it increases
the side population (stem cell) fraction of H460 lung cancer cells.[87]
Berberine, 300 mg three
times a day orally, also seems to inhibit complication of abdominal or pelvic
radiation, called radiation-induced acute intestinal symptoms.[88] The
studies suggest its use in clinical development may be more as a cytostatic
agent than a cytotoxic compound.
Berberine
reduces LDL cholesterol by upregulating LDLR mRNA expression
posttranscriptionally while downregulating the transcription of proprotein
convertase subtilisin/kexin type 9 (PCSK9), a natural inhibitor of LDL receptor (LDLR),[45] and increasing
in the liver the expression of LDL receptors through extracellular
signal-regulated kinase (ERK) signaling pathway,[46] while statins
inhibit cholesterol synthesis in the liver by blocking HMG-CoA-reductase. This
explains why berberine does not cause side effects typical to statins.
Berberine and plant stanols synergistically inhibit cholesterol absorption in
hamsters.[47] Rave
reviews on Amazon for controlling blood
surgark Available at amazon.com, 60 500
mg capsules for $15.00
|