The cholesterol hypothesis of heart disease — that saturated fat raises LDL cholesterol which clogs arteries — is not supported by the best evidence. The real culprits are fructose, oxidized polyunsaturated fats, and inflammation.
The Cholesterol Hypothesis
"The diet-heart hypothesis has been repeatedly tested and has repeatedly failed. It is time to move on."
"Ronald Krauss, MD"
The cholesterol hypothesis, promoted by Ancel Keys in the 1950s and 1960s, holds that:
- Saturated fat raises LDL cholesterol
- High LDL cholesterol causes atherosclerosis
- Therefore, reducing saturated fat reduces heart disease
This hypothesis has driven dietary guidelines and pharmaceutical marketing for 60 years. It is not supported by the evidence.
The Evidence Against the Cholesterol Hypothesis
Saturated fat and LDL: Saturated fat does raise LDL cholesterol. But it raises large, buoyant LDL (pattern A), which is not atherogenic. It does not raise small, dense LDL (pattern B), which is atherogenic. Fructose and refined carbohydrates raise small, dense LDL.
LDL and heart disease: The association between total LDL and heart disease is weak. The association between small, dense LDL and heart disease is strong. Statins reduce total LDL but have minimal effect on small, dense LDL — which may explain why their primary prevention benefit is so small.
Saturated fat and heart disease: Multiple meta-analyses have found no association between saturated fat intake and cardiovascular disease. A 2010 meta-analysis of 21 studies found no significant association.
Multiple meta-analyses have found no association between saturated fat intake and cardiovascular disease. The evidence against saturated fat was always weak — it was the food industry's preferred alternative to blaming sugar.
The Real Culprits
Fructose: Fructose raises triglycerides, raises small dense LDL, lowers HDL, causes insulin resistance, and promotes inflammation — all independent risk factors for cardiovascular disease.
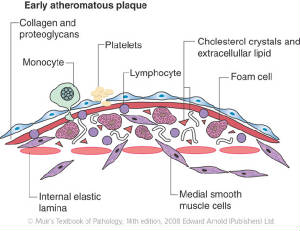
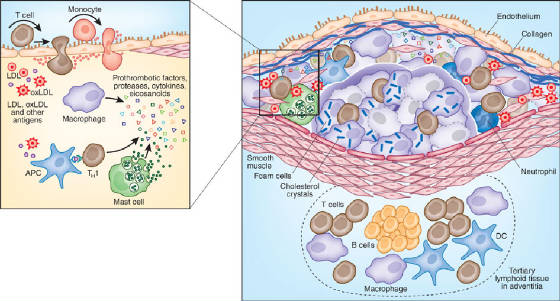
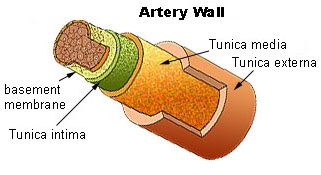
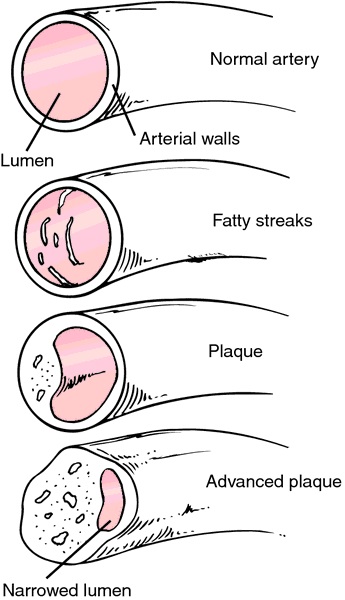
Oxidized LDL: LDL is not inherently atherogenic. It becomes atherogenic when oxidized. Oxidized LDL is taken up by macrophages in artery walls, initiating plaque formation. The primary cause of LDL oxidation is polyunsaturated fats (from industrial seed oils) incorporated into LDL particles.
Inflammation: Atherosclerosis is an inflammatory disease. C-reactive protein (CRP) is a better predictor of cardiovascular events than LDL. The primary drivers of cardiovascular inflammation are fructose, oxidized PUFAs, and insulin resistance.
The Statin Problem
Statins reduce LDL cholesterol by 30-50%. Their primary prevention benefit — in people without existing heart disease — is marginal. A meta-analysis of statin trials found that primary prevention with statins reduces the absolute risk of cardiovascular events by approximately 1% over 5 years. This means 100 people must be treated for 5 years to prevent 1 cardiovascular event.
The side effects of statins — muscle pain, cognitive impairment, increased diabetes risk, CoQ10 depletion — affect a significant proportion of patients.