|
Recommended non-technical summations |
||
|
Heart Conditions and Drug
Treatments --- 6/16/14 (http://healthfully.org/rns/id2.html
middle of page) The
causes for cardiovascular disease
(exposing pharma’s bad science: It isn’t cholesterol that causes
atherosclerosis and cardiovascular disease (CDV), but rather damage to low-density lipoproteins (LDL) through reactive chemical
(sugar or oxidation) and the
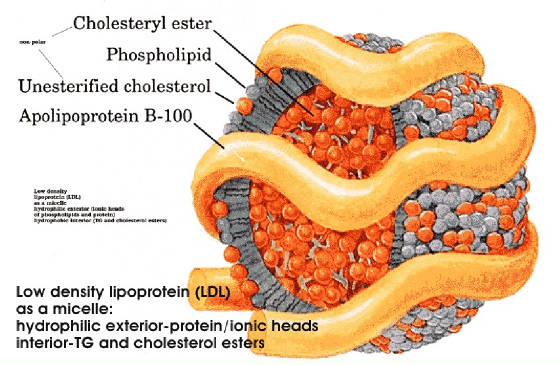
subsequent immune system response to the damaged LDL. LDL is the blood transport
system for
cholesterol and triglycerides in response to bodily needs. Cholesterol is vital for all cells. LDL is
water (blood) soluble complexes, and house approximately 1,500 cholesterol
molecules and 3,000 triglycerides. When
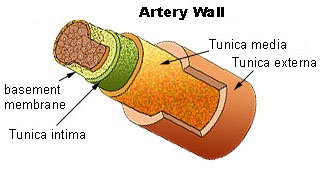
LDL that has penetrated the artery wall is damage by a reactive chemical
(especially sugar), two types of white-blood cells start the process of forming
plaque. This occurs in the Tunica media.
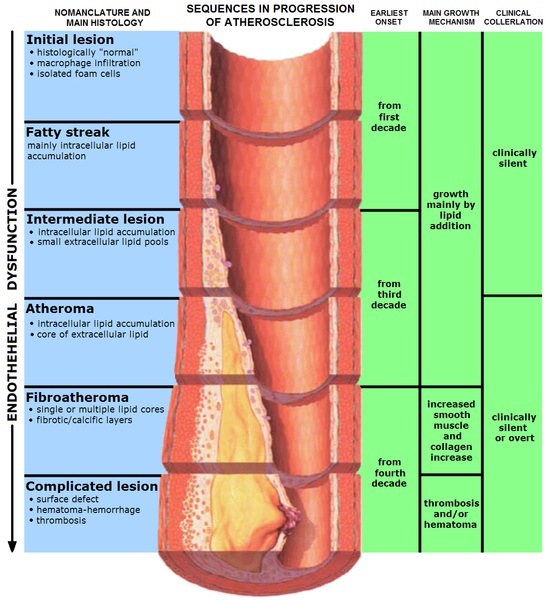
Over a lifetime the plaque accumulates and develops into
cardiovascular disease (CDV). Once
developed, the most one can do is try to slow its progression and allow the
body to slowly harden the plaque into a stable form and improve blood flow
through revascularization. Soft
YOUNG plaque that leaks causes 85% of the strokes and heart attacks. Thus cholesterol, triglycerides,
and LDL levels are moderately associated with CDV,
but they don’t cause CVD. The
liver produces more LDL filled with cholesterol and triglycerides inside it to
replace the damaged LDL. Pharma
wants doctors and patients to believe that statin family of drugs because they
lower cholesterol, triglycerides, and LDL that they can make a big
different—that’s B.S. Like
cholesterol, hypertension is a sign of atherosclerosis, and thus of increased
risk for adverse events, but hypertension is not significantly a cause of the
adverse events (with one exception: 15%
of all strokes result from a hemorrhage; and hypertension increases that risk).
|
|||||||
|
Drug Treatments Anticoagulants: They
are widely prescribed to prevent or treat thrombosis
(blood clots), which can damage the brain (stroke), heart (myocardial
infarction), lung (pulmonary embolism), and other organs. With a few exceptions,
they aren’t worth the
side effects. Pharma in junk clinical trials
exaggerates the risks of thrombi and the benefits
of their anticoagulants; their sales mantra is “safe and effective”. Pharma’s
opinion leaders use these junk
clinical trials to instruct physicians in the mandated continuing education
classes. Anticoagulants are routinely given to those who undergo major surgery,
hospitalized over 2 days, or have arrhythmia (irregular heart beat) because of
the higher risk of thrombosis. Once out of the hospital this treatment is
normally continued. They aren’t worth the
side effects. A much, much better choice
is to take a 325 mg of aspirin in the morning and another in the evening, and
it has many other health benefits (see aspirin above). At this higher dose it
is a better long-term
anticoagulant for preventing heart attacks and strokes (by about 50%), while
the low dose (thank you pharma) becomes ineffective over time because of
tolerance to its antiplatelet effect. At
this dose it also slows are stop atherogenesis. Aspirin also lowers the risk of most cancers
overs 40%, and for those with stage I, ii, or
iii cancer it lowers the risk of it becoming metastatic by over 40%. For these
reasons pharma educates doctors
about a grossly exaggerated risk of major bleeding, while in fact their
patented anticoagulants have a much higher risk. Long term ulcer risk at high
dose is 4%. Healthful life-style of low
carbohydrate-sugar diet and strenuous exercise
offers significant benefits because a poor flow of blood is the major causal
factor for a thrombi forming, and it lower s blood pressure another causal
factor for blood clots.
Arrhythmia (irregular heartbeat): is any of a large and heterogeneous group of conditions
in
which there is abnormal electrical [nerve] activity in the heart. Although
many arrhythmias are not life-threatening, some
can cause sudden death. About half of
sudden deaths occur during a major heart attack due to the destruction of heart
muscle. A basic problem with treating
an irregular heart beat with drugs is that they
are not magic bullets that just work upon the cardiac nerves and
muscles. They inhibit neurotransmitters
or the neural balance of minerals; thus upset cognitive and bodily functions. Arrhythmia
is a disease of mostly
seniors, especially those who have had a heart attack, and most arrhythmia
drugs are on the American Geriatric Society’s avoid list. Moreover,
they don’t stop arrhythmia (just modestly reduce them short term) and long-term
cause pro-arrhythmia (drug induced arrhythmia) thus
increasing death.
The evidence base for these drugs is broken since pharma does the
clinical trials for commercial gain. Other
treatments
include physical maneuvers,
electricity conversion, and electro or cryocautery are over sold. Arrhythmia
is used as a way to push anticoagulants
medication.
Their long-term usage has serious side effects. A far better choice is
325 mg of aspirin with
meals. Doctors
doing something is not the same as doing good.
For a heart
health learn about diet and
prevention of atherosclerosis. Hardening of the arteries (atherosclerosis, cardiovascular disease):
Cardiovascular
disease results from reactive chemical damage (especially glycation from
sugars) to LDL and VDL (the bad cholesterols) that stimulates an inflammatory
response in macrophages (a type of white-blood cell). They ingest the
damaged LDL. When too much they become foam cells that die
to form plaque within the walls of arteries that when sufficient become the
medical condition of atherosclerosis. Leaking plaque cause over 80% of strokes
and
heart attacks.. Healthful life-style of low
carbohydrate-sugar diet and exercise are the first line of defense. CoQ10 should be taken daily starting in the teen years. In addition
women starting with menopause and
continuing thereafter should take the natural
estrogen (estradiol), and men starting between 60 and 75 should take
testosterone. There is major
cardiovascular protection with estradiol; it is why cardiovascular disease and
heart attacks occur following menopause. Men on Testosterone are less likely to
develop metabolic syndrome (diabetes, hypertension, and atherosclerosis) and
are more likely to survive a heart attack.
Estrogen and Q10 protect LDL and VDL from reactive chemical damage, and
aspirin and estrogen inhibit the inflammatory process. As for Statins: pharma hypes its benefit and hides their side
effects. Lowering cholesterol has no
significant effect upon atherogenesis.
Aspirin, however, in the anti-inflammatory dose of 325 mg with meals or
greater prevents atherogenesis, cancer, Alzheimer’s disease, and
numerous other conditions. Thus pharma runs junk clinical trials and
educates doctors not to recommend an effective dose of aspirin. Aspirin, estradiol,
and Q10 along with
healthful lifestyle and low
carb-sugar diet can stop the formation of new plaque, and in most cases
over the years there will be a gradual lowering of risk for heart attack and
stroke as the body heals through revascularization. Heart Attacks (MI) and treatments: “Each year [2005] 1.5 million Americans
experience a heart attack and nearly 460,000 are fatal. Of those who die, almost
half die suddenly,
before they can get to a hospital” AHA. As with most acute conditions the list of
standard treatments, most are not worth the side effects. Following the
list below when the patient is
depending upon the help requires making the doctor aware of who is the ultimate
decider. With MI, there are two phases
acute and recovery. What works: Because tissue dies quickly, depending on
the degree of blockage, the PCI is modestly superior to the thrombolysis
(balloon angioplasty compared to clot-busting drug). The main benefit is within
90 minutes of
first symptoms. After 3 hours neither
procedure is worth the risks and side effects (as with all things medical the
benefits are greatly oversold and the risks understated). For arrhythmia there
are drugs not worth
taking, and physical interventions should be permitted only in the most serious
of circumstance. The drug best interventions
are nitroglycerine for angina pain and improved circulation, morphine for pain
and sedation, lidocaine for arrhythmia, epinephrine (adrenalin), and aspirin in
high dose, up to 2.5 grams per day as blood antiplatelet effect and
anti-inflammatory. All of these things
have been attacked by pharma using junk science trials and fed to doctors
through pharma’s thought leaders (see).
For recovery the typical well insured patient is treated long-term for a
variety of issues that cost on an average over $100,000 per year. Nearly all
of them have better
alternatives. CRITICAL CARE Effectiveness
of PCI
declines: it is significantly effective
in the first 1.5 hours from first
symptoms in lowering the death of heart muscle.
After 3 hours it is not
advisable because of considerable risks[1],
though guideline state 6 hours.
Thrombolysis (clot-busting drug) has a similar window of effectiveness,
though slightly less than PCI. Synchronized
electrical cardioversion can be
used to manages major arrhythmia and
major tachycardia (fast heart) if lidocaine
and morphine are inadequate. Implantable
Cardiovascular Defibrillator
(ICD) reduces risk of sudden
death. Again these treatments are given
to those who don’t benefit; those with typical, rather than major
arrhythmia. AVOID: (in order of
importance): downers (psychotropic
drug), Protein Pump Inhibitor (PPI), heparin
& other blood thinners, high blood pressure
medication except if extreme 180 over 110, antiarrhythmics except for
lidocaine, and oxygen. Downers (psychotropic
drugs) have many
indications such as anti-nauseas, muscle relaxant, sedative. If drowsiness or
mental confusion is a side effect, it is probably a downer (or an opiate). Some
have been approved for hypertension. Drugged, the patient is less likely to
inform
the nurse of a negative turn in their condition, or resist their doctor’s
advice. PPIs for acid indigestion are
addicting. Instead of heparin or similar
anticoagulant promptly take 975 mgs aspirin, followed by one every 4
hours. Drugs for hypertension other than
nitroglycerin do not lower morality Cochrane
Library and many of them are
downers. RECOVERY AVOID:
PPI is given with the
anticoagulant, but PPIs are addicting
because of the rebound effect, and long-term usage
causes serious life-shortening, side effects such as osteoporosis &
colitis. Tums, when needed, is a better
choice. Statins are totally over sold,
and are justified only by marketing
science. Counter to their marketing
science, they are not cardiovascular protective through they improved the lipid
profile and thus are not worth the side effects. PPI,
statin, blood pressure drugs, blood thinner, antiarrhythmics drug therapy, and
downer lack quality evidence that proves their net worth and superiority to other choices;
yet
they are routinely administered in the hospital and nursing home, when the
patient is most vulnerable. Avoid polypharmacy because it multiplies the risk of major side effects. All too often their side effects are treated
with additional drugs. All side
effects are grossly under-reported. Most drugs
started in the hospital and
nursing home will be continued long-term.
While recovering, avoid both stent and
bypass operation, they do not prolong significantly life, though they
reduce angina pain. “The vast majority of MIs do
not originate with obstructions that narrow arteries" Wiki. Coronary heart disease is caused
by atherosclerosis, with the young, unstable
plaque causing over 80% of the myocardial farctions. This results from damage
to LDL in the artery
wall which elicits an immune response.
Thus high level of cholesterol and hypertension are a result of atherogenesis.
Thus the best long-term way to prevent
subsequent MI is to prevent damage to LDL and lower the immune response. This
is effectively accomplished by taking
300 mg of CoQ10 and 325 mg of aspirin with each
meal. The natural estradiol 2mg lowers the risk for
women of MI by 50%, and testosterone should be taken sufficient dose to raise
the serum level to above 500 ng/dL.
Aspirin anti-inflammatory effect prevents at the high dose
atherogenesis, while at 325 mg per day lowers risk of blood clots. CoQ10 is
the best of antioxidants. Unfortunately the physician is not a reliable source of information,
his continuing education classes
are given by pharma; a pharma that does marketing studies to convince through
their opinion leaders that these off-patent drugs are ineffective and
dangerous. Hypertension results atherosclerosis (hard stiff arteries). The process starts with reactive chemical
damage (especially glycation from sugars) to LDL and VDL (the bad cholesterols)
that stimulates an inflammatory response in macrophages (a type of white-blood
cell). They ingest the damaged
LDL. When too much they become foam
cells that die to form plaque within the walls of arteries that when sufficient
become the medical condition of atherosclerosis. Leaking plaque cause over
80% of strokes and
heart attacks. The best way to prevent
or reverse hypertension is to prevent damage to LDL and the inflammatory
response. Hypertension
is a sign of atherosclerosis. Thus
lowering blood pressure has little effect upon the cause of strokes and heart
attacks—though pharma claims, of course, otherwise. Except for diuretics, pharma’s drugs to treat hypertension will
in general cause the heart to pump with less force or the arteries muscles
tissue to relax. These drugs in combination
lower cognitive function and physical strength and thus quality of life—three
of them are often prescribed. If you
must take a hypertension drug use a diuretic.
During a heart attack drugs that weaken muscles increase the risk of a
fatal outcome. Moreover, the prestigious
Cochrane review concluded
that:
“Drugs for mild hypertension have
not been proven to benefit patients.” Mild hypertension
is a systolic 140-159 and diastolic
90-99. Given that pharma runs clinical
trials and owns the results, bias
is the norm; thus the Cochrane conclusion is an understatement. Treating hypertension
with pharma’s drug arsenal (over 100 drugs of which 3 are typically prescribed
at one time) has serious side effects including drowsiness, cognitive
impairment, erectile dysfunction, muscle weakness, and low libido. Moreover,
pharma’s régime of drugs when taken
long-term doesn’t extend life. For
example the very popular group of calcium channel blockers cause a “higher
mortality rate over extended periods of use” Wiki--see also
Worst Pill,
and. “Beta-blockers are not recommended as first line treatment for
hypertension as compared to placebo due to their modest effect on stroke and no significant
reduction in mortality
or coronary heart disease” Cochrane.
Beta blockers inhibit CoQ10
(Q10). Ace inhibitors (5th highest selling class of drugs)
have
similar issues of side effects and likely fail to improve mortality
long-term. Clinical studies are all
flawed as to under-reporting of side effects, short duration and thus lack of
mortality figures—see Cochrane. The best approach (CoQ10, aspirin 325 mg, low
carb-sugar diet, and exercise) is the only reasonable choice. Long term prevention
of further development
of hardening of the arteries through aspirin 325 mg, Q10, low sugar low starch
diet, and estrogen will in most cases result in a gradual lowering of blood
pressure, and a significant long-term reduction in mortality. Follow heart recommendations which
treat the cause of HP, atherosclerosis, and those on diet (low carbs and sugars). This program will permit the body through
revascularization to lower blood pressure, eliminate angina, and dramatically
lower risk of MI. Revascularization is
a slow process. [1] Cholesterol embolism is very strongly
associated with invasive procedures: 20
of 22 patients in a histologically post mortem proven cases.
Cholesterol embolism issues became evident
with 3 months, most within 3 weeks, at. This cause of risk is rarely mentioned, and
if the adverse event occurs the physician will like attribute it to natural
causes, not their invasive treatment! Moreover,
the typical “Anticoagulant therapy appeared to exert an
adverse affect” at, and also at, which found warfarin a cause. |
|||||||
|
See cholesterol myth. For those who want to lower cholesterol, the
natural way is best: Niacin family and other natural cholesterol lowering drugs and cardiovascular
disease (CVD): Pharma recommends
1,500 to 3000 mgs of niacin (nicotinic acid) taken with meal; however insulin
blocks its cholesterol lowering affect.
High dose causes the unpleasant flushing and thus low compliance. The
only long-term study (niacin usage 6
years and effects followed an additional 9 years) was of high dose niacin. It
produced a reduction in deaths from
cardiovascular disease by only 11%.
However, a study based on blood work showed that 200 mgs of either
niacin or its inositol formulation taken at bedtime was just as effective at
lowering cholesterol, and without flushing.
In the same experiment similar results were obtained with inositol
hexanicotinate, a source of niacin.
Niacin also possesses anti-inflammatory and antioxidant benefits, and
thus inhibits atherogenesis. Phenolic
substances found in red wine are of value, as is nutritional yeast, red yeast
extract, and omega-3 fatty acids (found in fish and fish oil supplement) all
reduce risk of CVD. For lowering
cholesterol use 200 to 500 mgs
at bedtime of either niacin or inositol hexanicotinate. The reason niacin only
makes a modest
reduction in adverse events, and statin even less (once the bias of marketing
science has been removed) is because high
cholesterol is not the cause of CVD. But
rather it is reactive chemicals that
damage LDL and the subsequent immune response. This has been known for 4
decades and is
widely acknowledge in journal and Wikipedia articles. LDL, cholesterol, and
triglycerides are
essential for life; and saturated fats are health-wise the best source for
energy. Numerous scientists have exposed
the myth about cholesterol and triglycerides that pharma spreads. Pharma makes
billions selling drugs that
treat the symptoms of atherosclerosis. Treating them this way is as effective
as
treating the fever accompanying the flu with a drug that lowers fever. They
make billions more treating the damage
caused by a heart attack. However, as
explained in “Heart Issues”, the most important factor
for CVD is the inflammatory response
to damaged LDL, for which aspirin
and CoQ10, and estradiol for postmenopausal
women are truly protective. Testosterone past the age of 70 lowers risk of MI, heart failure, and metabolic
syndrome. Changes in lifestyle are very effective; especially regular strenuous exercise and eating a
low carb low sugar diet. If you must
lower cholesterol, then take 200-500 mg of sustained released niacin or
inositol hexanicotinate at bedtime. How can a drug make a damage heart muscle beat the normal
pattern? It can’t! To give
a drug to fix this problem based on a
surrogate outcome or improved ECC graph has been shown in the real world
population of patients to cause more deaths and heart attacks than those who are
not treated. Nevertheless cardiologists
routinely give arrhythmia drugs, they are following guideline.
INTERNAL SITE SEARCH ENGINE by Google
|
|||||||