|
Recommended non-technical summations |
||
|
Non-technical Summation
on MI & bad pharma -- 4/18/16
At http://healthfully.org/rns/id2.html
33-pageversion
of this with links to justify findings at http://healthfully.org/rhi/id1.html
1 long-page
of illustration and photos is at http://healthfully.org/rhi/id2.html
8-page, short
non-technical version is at http://healthfully.org/rc/id11.html
AMI Acute myocardial
infarction KOL
Key opinion leader AS Atherosclerosis MI
Myocardial infarction CVD
Cardiovascular disease PCI
Angioplasty balloon & stenting
Heart Attacks (MI) and treatments: “Each
year [2005] 1.5 million Americans experience a heart attack and nearly 460,000
are fatal. Of those who die, almost half
die suddenly, before they can get to a hospital” AHA. As with most acute conditions, the list of
standard treatments (listed in clinical guidelines), are not worth the side effects. There
is a seamless connection between bad pharma and their system of Key Opinion
Leaders (KOLs), and the production
of medical textbooks, university medical training, clinical trials, journal
articles, continuing medical education classes, guidelines, and why physicians
give junk treatments. The claimed
miracles such as angioplasty and bypass operations fail in quality studies to
extend life, and the drug interventions do even worse once the average positive
bias of 32% is subtracted[1] (remember
these 2
facts). Just about every clinical trial since the reforms started in
the corporate honor period, beginning under Regan is designed to promote
sales. Bias is good for business. Foreknowledge
of the corporate takeover of
medicine greatly increases the chances for you to understand why I won’t follow
the pharma treatment generated—through their KOLs—guidelines. I will let
my doctor or cardiologist know that I am calling the shots. My library of documentaries
and lectures
available on the internet will drive home the reality of “corporate honor”
while providing valuable information—Video
Library.
Pharma’s mantra is safe and
effective. Nearly all of the improvement in management
of cardiovascular disease (CVD) has
come through reduction in use of tobacco from 46% in 1960 to 16% today,
defibrillation, and the use of anticoagulants both during acute event and
during the recovery phase. We have been
fed a steady meal of safe and effective
as too the
physicians by an $800 billion global gorilla.
Having said that, what would I do for an
acute MI and for CVD?
To
start with allow me to explain SOME
ESSENTIALS. I have been a full time
college student for 11 years, spent over 40 years studying health science and medicine, and since 2004 been editing the healthfully.org website. A solid
foundation is essential for my making choices with a reasonable degree of
confidence. Most arrhythmia (irregular
heart beat) goes unnoticed and is quite common, especially among the
elderly. However there is
life-threatening arrhythmia for which little can be done unless in a hospital
and half of all those who die from a heart attack have this type and they don’t
make it to the hospital. Over 80% of
life-threatening arrhythmia is a result of damage to the heart muscles from the
lack of oxygen, called an ischemic event
also myocardial
infarction (MI) and AMI with “A” for acute.
Nearly all AMIs consists of two events:
first the leaking of young-immature
plaque (remember
this) from within the coronary artery. This
leaked plaque partially restricts the
blood flow, and then can cause platelets to aggregate around the plaque to form
a clot (called a thrombosis) that
cuts off the blood flow. Depending on the degree and duration of
blockage, this thrombosis type of AMI
causes heart muscle tissue to die within the first 60 minutes of complete occlusion
(remember this). Often this will produce symptoms of an AMI.
“Chest pain is the most
common symptom of acute myocardial infarction and is often described as a
sensation of tightness, pressure, or squeezing…. Pain radiates most often to
the left arm, but may also radiate to the lower jaw, neck, right arm, back, and epigastrium
[upper-middle abdomen], shortness of
breath (dyspnea) occurs when the damage to the heart limits the output of the left ventricle, causing left
ventricular failure and consequent pulmonary
edema
[fluid in the lungs]. Other symptoms
include diaphoresis (an excessive
form of sweating), weakness, light-headedness, nausea, vomiting, and palpitations and sudden death (frequently
due to ventricular fibrillation[arrhythmia]) can occur in myocardial
infarctions. Women also report more numerous
symptoms
compared with men (2.6 on average vs. 1.8 symptoms in men)”[2] Wiki. About half of
all AMIs occur to people without signs of cardiovascular CVD.
We are all at risk because we
could be forming young-immature plaque which is the type that leaks (remember this); and on an average those with CVD
are forming unstable plaque at 3 times the amount of those without CVD, thus
their higher risk. The typical young
atheroma (plaque formation) causes around 20% occlusion—not more than 50% (remember this). With
this little occlusion there are no
signs. It doesn’t even show up during an
angiogram (remember
this). This invasive imaging
involves a tube entering a main artery and being pushed up to the heart where a
dye is injected that shows up on x-rays.
These x-rays show only restrictions in blood flow of greater than 50% in
the major coronary arteries, thus it shows only the mature plaque with a
fibrous cap which won’t leak (remember this).
Think of the young plaque as being like an inflamed boil, while the
fibrous plaque is like a lump from a serval year old boil that now isn’t
inflamed. The cardiologist can only
treat what he sees, and what he sees with the angiogram does NOT leak to cause
an AMI.
Thus 1.5 million Americans yearly undergo a PCI (an angioplasty which
results in a sent being placed in a
coronary artery) or CABG (coronary
bypass operation) even though they don’t prevents heart attacks and
deaths. But those who undergo these
procedures are far more likely to take all the drugs his cardiologist
prescribes; far more so than the family doctor who is treating the patient for CVD.
If all the drugs the cardiologist prescribes are patented, their
wholesale price totals over $100,000 yearly.
Pharma knows how to butter its bread.
Since the cardiologist doesn’t have life-saving interventions, I
certainly wouldn’t go to one if I had CVD,
and if experiencing an AMI, I would not undergo an angiogram, which is one step
away from a PCI. One more very
important point, pharma has
doctors treating the symptoms rather than the cause. The disease is atherosclerosis
of the
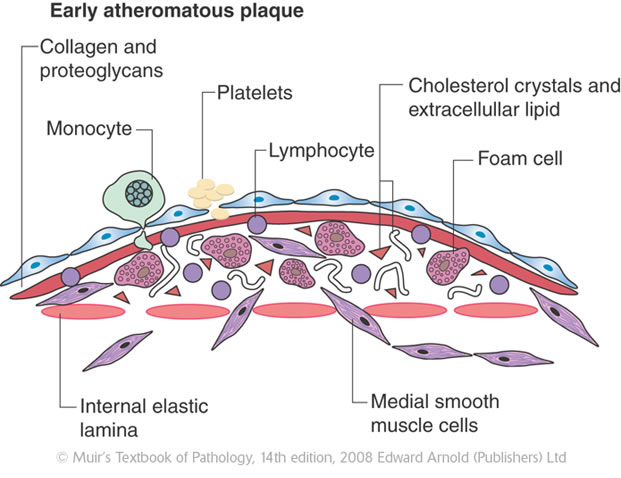
coronary arteries. This is caused by
pathogens living in the artery walls.
These pathogens cause an immune response which results in white blood
cells entering the muscular wall of the artery to attack the pathogens. To help
in rebuilding the damage, the cells
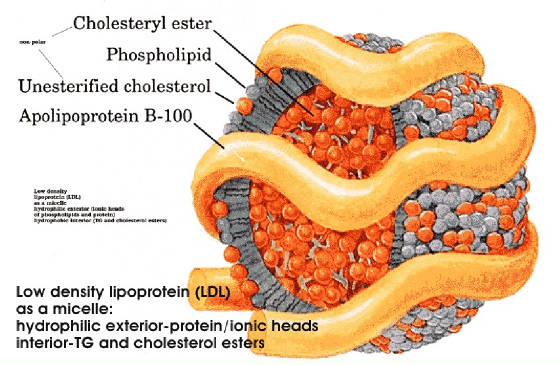
lining the artery (endothelial cells) permit the LDL to enter the artery
wall. LDL has a protein exterior and carries
cholesterol and fat (triglycerides) through the blood. The fat and cholesterol
are needed to build
the cell walls and membranes of the new cells that are forming as part of the
healing process. Fats and cholesterol
are good things, they are needed for cell growth. However, pharma makes billions
lowering the
level of cholesterol and LDL, and the food manufacturers make billions more
feeding us grains and sugars, both low in cholesterol and saturated fats (the
good fats). There is a chorus of critics
pointing this out. I suggest that you
watch the documentary put out by the Australian Broadcast Corporation, Hear
of the matter (part
1 & part 2, each 29
minutes); it will convince you that our media and the doctors pharma educates
have been feeding up crap. Or you can go to Amazon.com and enter cholesterol
myth. Pharma is in the business of treating illness, thus they treat
symptoms rather than the disease. It is
like lowering fever instead of using an antibiotic to help clear up
bronchitis—and statins are their most profitable family of drugs.
[1]
Positive bias averaged 32% (range 11 to 69%) for clinical
trials --NEJM article, 2008. The study
of neuroleptic drugs compared 74 journal articles to the raw data supplied the
FDA for phase III trials. Complete
records are required of these trials when pharma applies for a patent. This
data was obtained by 4 professors
through the FOIA (Freedom of Information Act). See http://healthfully.org/index/id9.html, or http://content.nejm.org/cgi/content/short/358/3/252 [2]
This is mainly due to size: tall people
have a bigger heart and bigger coronary blood vessels; thus complete blockage
by a thrombosis is less likely. This
results in less symptoms and greater survival rate.
|
|||||||||||||
|
WHAT
I WOULD DO: I would take
sublingually (under tongue for quick absorption) a 325 mg uncoated aspirin and
3 more with water, then take another under my tongue. I carry in my car a small
pill container with
20 aspirin. This use of aspirin is the
most important of all possible treatments.
Remember, that the second part to an AMI is the formation of a blood clot
(thrombosis), and the aspirin
at a high dose (325 mg) permanently blocks the action of platelets thus prevent
the clot. I also take a 325 mg daily
because it lowers the risk of CVD, AMI, and cancer very significantly.[1]
Atherogenesis
leading to CVD, its principle cause
is the Western diet with its large
amount of carbohydrates and fructose, this
combination screws up the liver to cause insulin resistance and carbs are
causal for endothelia cell dysfunction of those lining the arteries as is
smoking—link.
PCI (balloon angioplasty
with insertion of a stent) and thrombolysis when
administered in the first 90 minutes supposedly increases survival no more than 5%
(probably less); and
even then it isn’t worth the side effects. One real-world study showed
that only 1 in 125
patients meet this window of time from first symptoms to treatment. Because
of pharma’s control of the
information, including clinical guidelines, side effects are grossly
underestimated by cardiologist. For a
list of them, go to the in depth heart attack paper,
#s 17-24).
For arrhythmia the drugs are not worth taking, and physical
interventions should be limited to a pacemaker or defibrillation. The best drugs are nitroglycerine for angina pain and
improved circulation, morphine for pain, spasms, and sedation, lidocaine for pain
and arrhythmia, epinephrine (adrenalin) for low blood pressure and weak pulse,
and uncoated aspirin in high dose, up to 2.5 grams per day because of its blood
antiplatelet (clotting) and anti-inflammatory effects. (Note:
3.5 gram daily is the recommended
dose for arthritis--Merck Manual 1987,
p. 960, and prior issues.) Aspirin has been attacked by pharma
using junk
science trials and results fed to doctors through pharma’s key opinion leaders
(KOLs). For recovery the typical
well insured patient
is treated long-term for a variety of issues with drugs that cost on an average
over $65,000 per year. All of them have better alternatives. CRITICAL
CARE AVOID: (in order of importance):
downers (psychotropic drug,
sedatives)[2],
Protein Pump Inhibitor (PPI), heparin & other blood
thinners, high blood pressure medication
except if extreme 180 over 110, antiarrhythmics
except for lidocaine and morphine. Downers (psychotropic drugs) have many
indications such as anti-nauseas, muscle relaxant, sedative. If drowsiness or
mental confusion is a side effect, it is probably a downer (or an opiate). Some
have been approved for
hypertension. Drugged, the patient is
less likely to inform the nurse of a negative turn in their condition, or
resist their doctor’s advice. PPIs for
acid indigestion are addicting. Instead
of heparin, warfarin, or similar anticoagulant promptly take 975 mgs aspirin,
followed by one every 4 hours. Drugs for
hypertension other than nitroglycerin do not lower morality Cochrane Library and many
of them are downers. RECOVERY AVOID: PPI
is given with the anticoagulant, but PPIs
are addicting because of the rebound
effect,
and long-term usage causes serious
life-shortening, side effects such as osteoporosis & colitis. Tums, when
needed, is a better choice. Statins
are totally over sold, and are justified only
by marketing science. Counter to their marketing science, they are
not cardiovascular protective through they improved the lipid profile and thus
are not worth the side effects. PPI,
statin, blood pressure drugs,
blood thinner, antiarrhythmics drug therapy, and downer, all justified by
guideline though they lack quality evidence (more bad-pharma). Because
of guideline
all of these drugs are routinely administered
in the hospital and nursing home, when the patient is most vulnerable. Avoid polypharmacy
because it multiplies the risk of major side effects. All too often their side effects are treated
with additional drugs. All side effects are grossly under-reported. Most
drugs started in the hospital and nursing home will be continued long-term. While
recovering, I would avoid both stent and bypass operation, they
do not prolong significantly life, though they reduce angina pain. “The vast majority of
MIs do not originate with obstructions
that narrow arteries" Wiki[3]. They
are referring the hard mature plaque with
a fibrous cap, it doesn’t leak. Cardiologists are treating what doesn’t
cause
a heart attack; that is why PCI and bypass surgery don’t reduce mortality in
the real-world population. The plaque that
causes heart attacks doesn’t show up on the angiogram (angiography) so it can
be treated with surgery or stent. It is
the young, unstable plaque with less than 50% occlusion (typically around 20%). Thus
I would refuse angiogram which provides
the evidence that is used to sell the bypass surgery and stenting. The best
long-term way to prevent MI is to exercise
(see bottom of page at link). For the real causes for cardiovascular
disease go to rl. I now take 1,000 mg of CoQ10
and 1,000 mg of vitamin C daily because they
are antioxidants protect the arteries. I
also apply testosterone lotion
in sufficient dose to raise my serum level to above 700 ng/dL. As an androgen
it keeps my muscles including
my heart strong. The natural estradiol
2mg
lowers the risk for women of MI by 50%; my wife takes it. 325
mg of aspirin
has an anti-inflammatory effect that prevents atherogenesis, blood
clots, and also cancer, while
the baby aspirin is at 1 year useless because of tolerance. For
these reasons bad pharma teaches care givers that aspirin is so dangerous that
only the baby does can be safely taken. Unfortunately
the physician is not a reliable source of information,
reasons provide at beginning of the paper. The best thing I can do is
to do strenuous
exercise; I run, swim, and go to the gym. Exercise promotes revascularization,
which means that the body makes more coronary arteries because the heart needs
more oxygen. There are a number of
studies that prove its very significant benefits for seniors.
[1]
Your doctor is told that there is high risk of ulcer from aspirin, however it
is far safer than the anticoagulants hawked by pharma. Moreover long term
usage lowers the risk of
cancers over 40%. The low dose
recommended by physicians is ineffective because of tolerance and it is too low
to prevent cancers. Your physician will
not read this in the required continuing education class funded by pharma, nor
in the textbooks written by pharma’s KOLs.
See my paper on aspirin, on CVD protect, on cancer protection. [2]
They are given under a long list of deceptive names including muscle relaxants,
anti-nausea, anti-hypertension, anti-anxiety, antidepressants, anti-spasms,
anti-arrhythmia, and pain. If drowsiness
is one of its side effects, unless it is a in the opiate family, it is very
likely a sedative. Tramadol is a popular
downer (SSRI) whose claim as an analogic is based on a very weak opioid action.
[3]
A reaffirmation in Wiki, 2016 that the procedure dose not treat
the major cause of MI: It has been increasingly recognized, since
the
late 1980s, that coronary catheterization does not allow the recognition of the
presence or absence of coronary atherosclerosis itself
[namely the immature soft plaque that causes under 20% occlusion and 80%
of AMIs], only significant luminal
changes [over 50%] which have occurred as a result of end-stage complications
of the atherosclerotic process. See IVUS and atheroma for a better understanding of this issue” Wiki, 2016. So why are over a half-million patient sold
on its value???
|
|||||||||||||
|
6
clinical events in the exercise group and 15 in the PCI group
http://circ.ahajournals.org/content/109/11/1371.full,
Circulation 3109; 1371-1378, 3/8/2004
Percutaneous Coronary
Angioplasty Compared with Exercise
Training in Patients with Stable Coronary Artery Disease: A Randomized Trial,
Circulation--Hambrecht
R. et al.
Abstract
Background— Regular exercise in patients with stable coronary artery
disease has been shown to improve myocardial perfusion and to retard disease
progression. We therefore conducted a randomized study to compare the effects
of exercise training versus standard percutaneous coronary intervention (PCI)
with stenting on clinical symptoms, angina-free exercise capacity, myocardial
perfusion, cost-effectiveness, and frequency of a combined clinical end point
(death of cardiac cause, stroke, CABG
Methods and Results— A total of 101 male patients aged ≤70 years
were recruited
after routine coronary angiography and randomized to 12 months of exercise
training (20 minutes of bicycle ergometry per day)[1]
or to PCI. Cost efficiency was calculated as the average expense (in US
dollars) needed to improve the Canadian Cardiovascular Society class by 1
class. Exercise training was associated with a higher event-free survival (88%
versus 70% in the PCI group, P=0.023) and
increased maximal oxygen uptake (+16%, from 22.7±0.7 to 26.2±0.8 mL O2/kg,P<0.001
versus baseline, P<0.001 versus PCI group after 12 months). To gain 1
Canadian Cardiovascular Society class, $6956 was spent in the PCI group versus
$3429 in the training group (P<0.001). [This cost for exercise could be greatly
reduced
if after instructions by a physical therapist, the patient joined a local gym
and used their exercise bike, or bought one.
I have done both, and my costs yearly membership is $300 at LA Fitness,
and a quality exercise bike stand ran me under $275]
Conclusions— Compared with PCI, a 12-month program of regular physical
exercise in selected patients with stable coronary artery disease resulted in
superior event-free survival and exercise capacity at lower costs, notably
owing to reduced re-hospitalizations and repeat revascularizations.
In a large meta-analysis
that included 8440 patients in 32
trials, exercise training as part of coronary rehabilitation programs [for
those who had a PCI] was associated with a 31% reduction in the mortality rate
in patients with stable CAD/myocardial infarction.12 [The study above is compared exercise alone
to PCI.]
[1]
Those in the exercise group “participated in one 60-minute group training
session of aerobic exercise per week” full supra. This group session would
cause a greater
compliance of the daily 20 minute exercise part of the program.
INTERNAL SITE SEARCH ENGINE by Google
|
|||||||||||||