|
3. The weight regulatory system (WRS) and the
biggest losers: this is at the heart of why calorie
restricted diets fail; the system turns on to preserve the adipocytes set level
of fats stored through hormonal regulations of which 6 are produced in the
adipocytes. The other barrier is that
with IR the adipocytes, depending on degree of IR and social environment, will
reset as weight is gained after a period of time (I guess at 1 to 2 years depending on age,
hormones, fatty liver, and physical activity). Once set, the WRS will cause the regaining of weight for years
until the set point has been reach, and depending on the degree of insulin
resistance can cause continuation of weight gain after reaching the old set
point.
Free-living
humans are especially vulnerable to the effects of obesogenic environmental and
behavioural pressures, which pose a significant barrier for the continued
success of weight-loss attempts. This is further compounded by elevations in
metabolic efficiency (whereby energy expenditure declines beyond that predicted
from the change in metabolic mass) and
appetite
which accompany weight-loss, and may ultimately predispose to weight
regain. Moreover, changes in neural activity
within brain regions known to be involved in regulatory, emotional and
cognitive control of food intake have been observed following weight loss.[1]
This
process of regaining has been called the
yo-yo diet. Caloric
energy restriction (CER)
has been shown to work year after year in a TV contest, The Biggest Losers. In a boot-camp
for the obese, contestants compete for cash.
They are on the healthful standard “move more, eat less” program.
There were 16 contestants in the 2009 season
of which 6 men and 8 women agreed to participate in the follow-up study 6 years
later. These 14 lost an average of 38%
of their weight, 127 pounds over the 30-week show. CER works for contestants,
but for how long?
In
the Journal article and New York Times articles on The Biggest Losers, it
showed that they at 6 years the 14 had regained 71% of their weight, and
“Weight regain was not significantly correlated with metabolic adaptation at
the competition's end (r = −0.1,
P = 0.75), but those subjects maintaining greater weight loss at 6 years
also experienced greater concurrent metabolic slowing (r = 0.59, P =
0.025).”[2] The averages at baseline were 35 years,
weight 327 lbs., BMI of 49.5, percentage fat 49%, At end of show, 30 weeks,
weight 199 lbs.,
BMI 30, percentage fat 28%, Weight gain
at 6 years would have been a greater if they excluded the one contestant, Rudy
Pauls, who prior to surgery had regained 167 lbs. Rudy after bariatric surgery
lost 102 pounds,
thus at 6 years he was just 65 heavier than at end of show. His metabolism at
the end of the show had
dropped by 804 calories, after surgery it was 520 calories less than baseline 6
years before.[3] Excluding Paul, only one contestant at 6
years their basal metabolism had improved compared to at the end of the show,
the other 12 had a further decline in metabolism than week 30. The contestants
6 years later eat hundreds of
calories less than people of a comparable size just to maintain their new
size. All 14 contestants at 6 years had
a decline in metabolism. At 6-years for
Mark, his metabolism was 525 calories below at the start of the show. Only one
contestant, Erinn Edbert, kept the
weight off (and afterwards lost 25 pounds more), but her metabolism dropped at
end of show just 30 calories, but at 6 years it was 570 calories lower than
baseline. This is about 30% less
calories to maintain her weight loss.
She was the only contestant to continue to lose weight. Danny Cahill,
the biggest lost 235 pounds of
which he restored 105 pounds by the 6th year. All the contestant
experienced a very
significant reduction in metabolism at the 6-year mark, their WRSs were still
functioning to cause weight gain.
The processes are controlled by hormonal systems
designed through evolution to promote survival.
Slow starvation as supported by the example of the Biggest Losers show that
CER is for the long-term overweight
a fix that fails. What is known as the yo-yo
diet.
There are hormones that regulate weight, and if the
system has been rest to 350 pounds, it will function to maintain that
weight. In a social environment those
controls can be overridden. Remove the
social environment, the boot camp, and the controls again dominate. How much
weight depends on both how much
repair occurred during the boot camp, and how much.
4. Blaming the
victims:
Industry and their puppets blame the victim, and not the food
manufacturers. In the UK the BBC has
done a series of documentaries exposing the role of the food manufacturers who
put profits before people, the same has been done in Australia and Canada, and
I assume in the other European countries.
So what are the major ways to blame the victims in the US?
The weak-willed
yo-yo dieters: an example is all but one of the Biggest
Losers. Ignored is Leptin and
the other hormones that control appetite and metabolism. The second errors is
that the brain doesn’t
and the hormones that regulate functions are not controlling. The weal-willed is based on a theory that the homunculus
(commonly called a soul or mind) controls
behavior over the hormonal regulatory system.
The neuroscience has shown that the brain is in charge, but the common
mimi[4] is
that the homunculus/soul is the decider.
I will resist going into neuroscience, but recommend Free
Will and Free Won’t at http://www.skeptically.org/spiritualism/id11.html. The brain
rules, including what is thought and said.
That the rational module isn’t aware of the brain functions promotes the
illusion that it is in control. It is
part of the input for what is done, but it isn’t the decider. I will leave
you with that proposition since
it is beyond the scope of CAWD.
Those who succeed, which for long-term overweight
is
under 10%, occurs because of details not mentioned, such as bariatric surgery,
extended fasting (#7), amphetamines, illness,
chemotherapy that
damages the digestive system, and others less common. The example above of Mrs.
Errin Edbert mainly
turns upon the relief of boredom caused naturally by the reduction in the rate
of metabolism. The reduction in brain
and physical activity is popular not just among HSPs and LSPs, both populations
which have a significant numbers of those who regular take substances such as
ethanol, marijuana, and neuroleptic drug, and among the paleo there is a long
list of herbal drugs,[5] Mrs. Edbert in the biggest losers, her brain
chose the body’s way of relieving boredom, which was probably supported by the
social environment. Sure, the rational
module[6]
contributes, but it doesn’t control.
Everyone knows that smoking shorten life and reduces its quality; thus
if reason ruled there wouldn’ t be cigarettes, pipes, and cigars.
Gluttony and
sloth are commonly used to
explain why people gain weight and retain it.
The phrase is used as a character description. It could be caused by
inheritance or by the
mind, which thus is another way to point the blame the victim for the above
weak will. The inheritance is to blame
their genes, a version of the thrifty
gene theory. This explanation
excludes the food manufacturers, media, and blames the victim.
Thrifty gene
theory merits more space since
those who should know better, don’t, including Robert Lustig and Richard J.
Johnson (see bibliography) for their books--both books of high quality by
widely published authors. It is a
popular excuse for why we get fat, the genes made us. This implies that we have
a system different
than other mammals.
Genes are used to explain the failure to lose
weight. She has thrifty genes; thank-god
I wasn’t born with them! Her
body is programmed to store fat to promote survival during a food shortage;
that is why she puts the weight back on.
This theory assumes there is a survival advantage during scarcity of
food thus the genes for being overweight are selected for among Homo sapiens;
but is there.
First, it is unlikely that the paleo
ancestor would have zero food. These
hunter-gatherers have secondary, less-favored sources of food during draughts
or other events affecting their food supply.
Starvation is not common. Second,
the news reports of famine are
not among the paleo peoples, but the areas which depend on farming with a
typically 10-fold denser population. Third
there isn’t a mammalian model for
thrifty gene: when there is plenty of
food there isn’t obese species, expect by design. Design such as when
there is long migration
or hibernation. The mechanism for
increase fat is through insulin resistance,[7]
and there is a biological clock.[8] Weight is so important for survival that the
palate doesn’t control it. That since
doesn’t cause morbid obesity in mammals, and they can lose the weight after
migration or hibernation. Why can’t
we. The only explanation that fits the
facts is that our WRS on a cellular level is broken.
An obese person is a target for arrows, stones, and
spears, common causes of death. Obesity
is selected against, unless it promotes survival as in cold climates for the
whale and walrus, or for sexual selection, the male walrus. A broken system
causes obesity.[9] The Rhino, hippo, and elephant have muscle
and thick hides, not large stores of fat.
I too have a thick hide that protects me from casuistry of all
types. Through sexual select obesity
is strongly selected against, On
top of that a person with an extra 50 lbs.
their risk of death by 50%.[10] A
thrifty gene would be strongly selected against.
An addition to the theory of thrifty gene is added
by
Richard Johnson who combines the uricase gene deletion which occurs in apes and
guinea pigs. He argues that during the
ice age there is a selective advantage to the deletion of the uricase gene (4:1, 6, also known as urate
oxidase), which causes a higher level in the apes of uric acid. The effect
of the deletion is higher uric
acid which Johnson proposes causes increased conversion of fructose to fatty
acids—a plus during the ice age with scarcity of food. “The Uricase
Mutation enhanced the ability of
fructose to increase fat stores and insulin resistance.”[11] For a researcher with both skills in writing
and analysis this is a howler. First,
the mutation occurred first among the tropical apes, who were not subjected to
the ice age and long before the split to from homo Sapiens. Second, the elevated
uric acid causes
increased DNL is less than certain, since DNL is a response to inadequate ATP;
thus the role of uric acid in production of ATP hasn’t been confirmed. Fourth,
Why would the guinea pig also have
that mutation (and possible other untested mammals). Fifth, articles on uricase
suggest that there
was based on current primate population a decline in uricase activity among
many of the primates. Why have hominids
gone one step further, the mutations removing uricase production? Sixth, the
Wikipedia article and other
suggest that the increased uric acid was for its antioxidant action. “Uric
acid is a powerful antioxidant and
scavenges of single oxygen and radicals.
Its presences provide protection from oxidative damage, thus prolonging
life and decreasing age-specific cancer rates.” [12] This wiki article analysis fails for the
other hominids aren’t that long-lived, other mammals are long lived without the
mutation, and the guinea pig is short lived.
The uricase mutations remain a mystery, for which Johnson’s solution
falls short. We all at times fall on our
face. His The fat switch is among
the best of books on western diet and diseases.
5. Three types
of diets: caloric energy restriction, low fat high
carbs, and Atkins-keto diet: As covered above the caloric
energy restriction (CER) has few
successes because the WRS increases hunger and reduces metabolism. Heads on
studies comparing low carbs to high fat diets have shown that fat is better
than carbs. Moreover, compliance is low
in the CER diet because of leptin increasing hunger and making the dieter
feeling crappy and moody because of the reduction in the rate of
metabolism. Life-long changes in diet is
an issue with diets. CER is seldom a
lifestyle change because of the action of leptin, and the low carb Atkins-keto
diet because of social pressures and simply put sugar and carbs taste good to
us—but not to carnivores.
The western low fat diet is life-long,
or
should I say, life shortening? The
low fat and low cholesterol diet is
the food manufacturers wet dream, less eggs, meats, expensive saturated fats,
and more carbs. Low fat foods are bland;
mother nature wants us to eat plenty of fats--as most paleo peoples do. To improve
flavor, the food manufacturers
have upped the sugar, for which by biology there is a reinforcing response in
the brain, and sugar is much cheaper than vegetable oils. The net result of
the high sugar diet that
causes insulin resistance, and with that is weight gain and increased
calories—more sales. And pharma profits
from the pathogenic pathway.
The assault on the American diet
has been
going on for over a century by the Sugar Institute and food manufacturers, and
we are seeing the toxic results.[13]
In the widely
reported A to Z trial, which was
published in the JAMA, compared low
carb with high fat and proteins to 2 energy restricted diets with varying
amounts of protein and fats and the LEARN program of exercise and eating less. Atkin’s
(Keto) diet doesn’t restrict
calories, only carbs, while the others restrict calories and the Zone diet is
higher in fat but less than the Atkins, and with moderate carbs. The Ornish
diet is a very low fat diet, and moderate
protein, very high carbs vegetarian diet.
The results hands-down favored the Atkin’s diet averaging nearly twice
the weight loss.
In this major head to head study
funded
by the NIH, 4 popular diets were compared in a randomized 1-year trial with
1-year follow up, conducted from 2003 to 2005.
Three hundred and eleven free-living overweight/obese, non-diabetic
premenopausal women were assigned to one of 4 diets. Atkins, LEARN, Ornish,
and Zone diets.
Diet and Physical Activity Data. Dietary intake data were collected by telephone-administered,
3-day, unannounced, 24-hour dietary recalls using Nutrition Data System for
Research software, Versions. . . The recalls occurred on 2 weekdays and 1
weekend day per time point, on nonconsecutive days whenever possible. A “food amounts
booklet” was u sed to assist participants with portion size estimation. Energy
expenditure was assessed using the
well-established Stanford 7-day physical activity recall.
In
all 4 diet groups, 85% to 89% of participants attended at least 75% of their
assigned classes.[14]
Only the Atkins diet did
not require energy restriction; even so the kcal/day was within the range of
the other 3 diets—protein and fats have a higher satiating score than the
carbohydrates and therefore a reduction in calories and an even greater
reduction in ATP because Atkins is also a high protein diet and also because
per calorie the ATP production of fats (rated at 10 calories per gram is less
than for carbohydrates rated at 4 calories per gram.[15]
Surprising
to the Stanford group who administered the trial, the Atkins group lost over
twice as many kilograms: 4.7 for Atkins
and 2.2 average for the others 3 in the trial.
The trial lead Prof. Christopher Gardner of Stanford, a vegetarian, spun
the conclusion to support his belief: “While questions remain about long-term
effects and mechanisms, a low-carbohydrate, high protein, high fat diet may be
considered a feasible alternative recommendation for weight loss.” (supra,
969). Why not say, given those numbers
that the Atkins diet had twice the weight
loss of the four popular diets?
On looking at the dietary numbers these results are strong
evidence for the conclusion that strict adhesion to the Atkins diet for most is
not necessary and that with a mere 22% increase in calories from fat and a 289
calories less per day they lost more than the other 3 CER diets with normal
carbs or increased carbs. Fats for the
Atkins went at baseline 36.2% of calories to 44.3% at 12 months and calories at
baseline went from 1888 kcal/d to 1599 at 12 months, a 15% reduction in
calories.” [16] The numbers were similar as to calories and
energy expenditure at baseline compared to 12 months for all 4 diets.
All
the diets showed significantly greater adherence at 2 months, but by the 6th
month adherence significantly declined.
This is consistent with many, many other diets, in that around 2.5
months, leptin levels change to conserve fat, and weight loss is modest
thereafter. The point is that that
increasing fats and staying with low sugar is the big difference. Those on the
Atkins diet would have had lower
sugar at 12 months than the other 3 diets (though not measured in this trial,
which swallowed the lipid-cholesterol fallacy).
Those with the greatest IR would have to notch up the adherence, and I
would recommend increasing the fat and dropping net carbs to about 15% of
calories or less if need, and adding intermittent fasting, and the worse cases
would need to add alternate day fasting (#7-8). In other words, they would need to stay
longer in the fat metabolizing and autophagy phases.
I smell a KOL not just from
what he said and his being selected
as lead author. Christopher Gardner is an
outspoken vegetarian. Second he could
have selected the top quintal of each group for comparison, since those would
have the greatest compliance which given the protocol of the trial is a
significant issue. Third, it is common
for those with a bias to spin both the conclusion and the abstract, which is
what I found. Fourth our government’s
record of health science is in support of industry, with a few exceptions. Is
this an exception?
9 The
numbers for the carbohydrate consumption of those on the
Atkins diet indicate very low compliance and compliance given that major weight
loss requires ketosis. “Fats for the
Atkins cohort went at baseline 36.2% of calories to 44.3% at 12 months and
calories at baseline went from 1888 kcal/d to 1599 at 12 months, a 15%
reduction in calories.” [17] The numbers for fat of those on an Atkins
diet should have been around 70% with about 25% protein and 5%
carbohydrates. Overall compliance was
not just poor in this self-reporting study for Atkins but also for the LEARN,[18]
Ornish, and Zone diets.[19] The first 2 months of the Atkins diet followed
the recommended 20 grams of carbohydrate (5%) for the induction phase, and
raised to 50 grams per day for the subsequent 10 months which is 12.5% of
calories from carbs. However, assuming
25% of calories from proteins, the average carbohydrates is 31% or 124 grams a
day, 2.5 times the 50 grams allowed in the maintenance phase. A study of the
compliance of the 232 women in
the A to –Z trial found, “Given these low
numbers, no further data are presented comparing absolutely adherent vs
nonadherent participants. . . . In general, absolute adherence to all three dietary
guidelines was very low.”
[20] Note
the
ketogenic diet, such as used for intractable epilepsy is at 5%, as too diet for
starving cancer. Thus the high amount of
carbs under-estimates the effectiveness of the Atkin’s diet; that amount of
carbs causes a Randle cycle switch that reduces metabolic rate, not just fat
metabolism, typically during the 2nd month of the diet. The A-to
Z comparison study conforms to other
that show in the real world a compliance is low.
Gardener
is not the only Professor to let his beliefs cloud his reasoning
processes. In the Scientific American of
2015, a full article was written in response to Dean Ornish’s in the New York
Times. They gave the task to their
science writer:
Ornish
goes to argue that protein and saturated fat increase the risk of
mortality and chronic disease. As evidence for these causal claims, he cites a
handful of observational studies. He should know better. These types of
studies—which might report that people who eat a lot of animal protein tend to
develop higher rates of disease—“only look at association, not causation,”
explains Christopher Gardner, a nutrition scientist at the Stanford Prevention
Research Center. They should not be used to make
claims about cause and effect; doing so is considered by nutrition scientists to be
“inappropriate” and “misleading.” The reason: People who eat a lot of animal
protein often make other lifestyle choices that increase their disease risk,
and although researchers try to make statistical adjustments to control for
these “confounding variables,” as they’re called, it’s a very imperfect
science. Other large observational studies
have found that diets high in fat and protein are not associated with disease
and may even protect against it. The point is, it’s possible to cherry-pick
observational studies to support almost any nutritional argument.[21]
Moyer then goes
on to give some of the evidence that fats are heart healthier than carbs (which
includes gobs of fructose on the western diet).
For those who like the video format a
series of educational, mostly excellent coverage of topics, which averages 16
minutes, with excellent supporting video materials, done under the pseudonym of
What I’ve Learned, with a number of them on diet. This one covers the
crapolla of Harvard
professor Kim Williams whose references to his meta-analysis doesn’t support
his claims
***** Obesity and diabetes explained: the
overflow phenomenon 16 min, 538,000
views, Oct 2018, What I’ve Learned. Starts with history, good basics such
as
insulin causes fat storage, and rebuttal of bad studies, but failed to mention
industry funding or going into the biology behind ketogenic diet—covered
elsewhere. He shows how KOLs lie to the public & physicians https://www.youtube.com/watch?v=xlfZvnV4v50 Excellent Part
II is
Can you cure diabetes/does fat cause diabetes
Of the gems in this 16-minute video,
it takes to task the claim of Harvard cardiologist Kim Williams who, said “No
one should be doing the ketogenic diet. It
is an article with Williams quote as title Sept 5, 2018,[22]
and with over forty reference in support of the meta-study. He supported this
statement by a meta-analysis of 17 studies—sounds good! The claim was
based upon the finding that the
low carb diet increased heart conditions and mortality. Seventeen of the studies
his studies were based on questionaires, moreover, none of these studies
mentioned a ketogenic diet. One of these
studies Kim used wrote in its conclusion:
“Our results do not support a clear, general association between LCHP
score and mortality.” Four studies
showed better outcomes with low carbohydrate diet. Eight of the studies used
did not specify the
amount of carbohydrates consumed. The
ten studies that specified amount of carbs well above the level for a ketogenic
diets. Low carb is 10% of calories, and
ketogenic 5%. The lowest of the studies,
2 of them were 25% of calories from carbs, and the remaining 7 studies were at or
above 30% carbs, which is 6 times higher than ketogenic diet. In summary Williams
deliberately lied in his
published meta-study. What percentage of
the readers will check his references?
What percentage of reader will assume the evidence supports the standard
recommendations of move more, eat less, less fats, and that the popular
ketogenic diet is just another fad diet?
Very few readers have the background to recognize his tobacco science.
While the ketogenic diet has taken
off
like the Atkins diet of 40 years ago. They
are brothers in that both are very low
carbs (5 to 10% for the keto & Atkins diets), and thus high in
fats. At above 10% of calories, I would
not consider it an Atkins-ketogenic diet because of the carbohydrate’s effect
upon ketosis (fat metabolism). It is
thus important to stay in the under 10% range, because of what is called the keto
flu, a period lasting several
hours. I call it hitting the wall,
referring to when an athlete runs out of
energy. Going in and out of ketosis has
this price.[23] It is part of the body’s adjustment to fat as
the only source for the production of ATP, a metabolic switch conserve ATP
occurs during the switching process. One way of avoiding it is to start with a
36 hour fast.
The new Atkins diet which limits
proteins, I find the science for it flawed (#9),[24] and
would have a lower rate of adherence.
With less protein, there should be a lower adherence in the New Atkins
diet. Proteins have a higher satiety
rating, and fill as the pleasing the palate the gap left by carbs from breads,
beans, etc. The quick boost in energy
from digestible carbs is a strong reinforcer, thus satiety reduces the hunger
for carbs. As for adverse health
consequences of high
protein, that hasn’t been shown by quality studies.
This pattern of
very low carbs reminds me of the niacin
story for lowering cholesterol. The
official recommendation is a high dose,
1,500 to 3,000 mgs which causes unpleasant flushing lasting about 10 minutes,
and the peak level of serum niacin is half hour, with half-life under one hour. Moreover,
cholesterol is made by the liver at
night, and over 70% of cholesterol is produced by the body. Thus few will follow
the recommended niacin
treatment for hypercholesterolemia.
In my extensive research lasting
over
2-months on niacin and its related compounds, I found out that cholesterol
medications should be taken at night. A
study in the 1960s followed that in their protocol in a clinic where blood
levels of cholesterol were measured during the night for the cholesterol lower
effect of niacin and 3 other related compounds.
I knew that the liver makes cholesterol at night, when other metabolic
and catabolic demands are low, but I hadn’t realized what that entailed until I
read the article. Thus by 2010, I had
concluded that a low-dose, slow release at night would be more effective than a
high dose of niacin (or a statin) in the daytime. See http://healthfully.org/rc/id4.html
for my extensive research on niacin.[25] So why would the standard be 3 grams of niacin
with it side effect of hot flush feeling lasting about 15 minutes. This creates
a compliance issue. II see this pattern repeated with the keto
diet, very low carbs-creates a compliance issue.
I also believe, on weak journal
evidence,
that mega niacin has antibiotic property.
A journal article so stated and the high amount made by yeast, supports
such antimicrobial action. On that
basis, with the excess niacin excreted in the urine, it might help cure a UTI
(urinary-track infection) depending upon strain of bacteria. The colony
might exist in tissue not exposed
to the high concentration of niacin in urine.
The best and safest treatment are the sulfa drugs. I tell you this because
the physician’s
computer directing his prescription writing won’t mention sulfa drugs—it is up
to the patient.
Back to the
question of best diet. During the weight loss phase, carbs
should be kept at a
minimum. On weak evidence, but personal observations and journal articles
and books, they have caused me to believe that a diet of 85% of calories from
fat (not counting proteins ) and 15% from carbs in the maintenance phase works
once the youthful weight has been obtained.
If weight is gained than lower carbs.
One reason
is that consumption of a modest amount of carbs won’t throw the Randle cycle switch to fat storage.
Some of the evidence in support of this
hypothesis is that following bariatric surgery, during the first two weeks the
diabetic make major improvements, some of whom are off their diabetic drugs. Secondly
the success of Michael Mosley’s diet
plan (see bibliography) based on his combination of fasting (#7).
It permits during fasting days 500 calories for women, and 600 for
men—no restriction on carbs (I think there should be). His plan (book
was an international best
seller) has a much higher long-term compliance than a ketogenic diet. More
research is needed on the level of insulin, proteins, and
carbs that operates the Randle cycle, and also the hormonal changes that affect
metabolism and appetite.
In fact, I find Atkins works with
its
maintenance phase effective, but most drift back to excessive carbs, and like
in the The Biggest Losers (#3) regain
slowly their weight. The New Atkins diet
claims that moderate protein produces superior results, a change that I find
the evidence lack and contrary to evolutionary biology and the androgenic role
of insulin (#9).
Atkins is high protein
and high fats. Atkins recommended that
once the lean weight is obtained, that carbs can be gradually be reintroduced
to the point where weight is gained. At
that amount of carbs, (say 25% of calories, then back off about 5% so not gain
weight. The New-Atkins Diet recommends
no more than 20% of saturated fats, thus high in the rancid PUFAs—stupid ignorance
of the science and catering to popular belief (4:4, 4).
I have seen over and over again
those who
have not followed the maintenance level recommendation and have gained most of
their lost weight. I have seen the same
with the Medfast diet, once off the plan the WRS restores gradually the
previous level of obesity. Medfast is a
very low calorie, low fat diet, with prepared foods and powder mixes and weekly
counseling. We live in a toxic social
including media environment, and the research on yo-yo dieting is often just
number gathering. There is need for research as to when the
leptin and other hormones stop operating for gaining weight and the cause for
this change. Observational studies need to go beyond
numbers gather and examine hormonal changes that cause weight gain.
Dieting has a very
low success rate for those with long-term excess weight of more than 20% their
lean body weight. We have reviewed the
failure of The Biggest Losers (#3),
the modest results of the A to Z trial
(#5), and we
all know of the yo-yo diet. Not all is
gloom: bariatric surgery has been able
for some to bring about long-term weight loss and for most to cure t2d. Does
the same apply to the ketogenic
diet? Does it get past the hormonal
regulatory system?
Atkins-Ketogenic diet: Beyond the A to Z trial, ketogenic diet has consistently
outperformed the calorie restricted diet. It is simple, limit net carbs to 50
grams a day or less (net carbs are total carbs minus fiber). “The
original KD was designed as a 4:1 lipid:nonlipid ratio, with 80% of daily
energy intake from fat, 15% protein, and 5% carbohydrate.” [26]
In 6:4 #4
the many health benefits are
listed. These benefits come from turning
up the healing processes, autophagy, by maintaining low insulin (6:1).
As for weight loss, those that adhere to it have the pounds melt
off.
A neighbor and friend of mine in
under 4
months, from September through December of 2019 lost 38 pounds. I saw Margret
regularly and often walked with
her and her 2 dogs. She told me that
this was her third time on the Atkins diet, the first time she weighed 219
pounds. Margret at the age of 38 lost a
pound a day and in less than 3 months returned to her youthful 135 pounds. I
found that hard to believe, then accepted
it based on my observation of her weight loss in just under 4 months, where she
has gone from 178 to 140. Her normal
weight at 5’9” is 135 pounds. At the age
of 63 she said this time was significant more difficult, took longer. Margret
said the hardest thing was giving up
eating fruits. She understood the
biology behind the ketogenic diet. I
didn’t have to explain mitochondria and ATP.
She understood that with declining MTD functions the rate of weight loss
was slower this time around.
I did explain to her about autophagy,
Ketogenic
diet turning it up, and the metabolism of the excess fat in the liver and
pancreas; science not in the books on ketogenic and Atkins diets. I suggested
a morning fast, and she told me
that she normally skips lunch. It makes
me smile inside to know that some people see further in my senior
community.
Another neighbor has done the same. Started near the end of a bout of
gastroenteritis.[27] Having gained about 20 pounds over the last 10
years she went on an Atkins diet.
Stephanie’s 5-months of general malaise and stool problems was
cured—possible helped by her change in diet. Within 3 months she had lost
the excess pounds,
at 5 foot 1, 20 pounds shows up.
Adherence has two
foes, that of the social environment, including a mead loaded with food ads and
cooking shows. The second is that of a
craving for carbohydrates mainly because of extreme low carbohydrates requires
the glycogenesis in the liver to supply the needs of the most common type of
cells, the erythrocytes which lacking mitochondria, rely upon fermentation in
the cytosol to produce ATP—there is no process in the cytosol for the
production of ATP from fats.
As for the weight
loss on an Atkins type diet the evidence in journals is on short-term, trials,
all with the major issue of compliance, and lacking tracking participants for
more than a year. Except for tobacco
science, significant funding for decisive trails has not been available.
The best I could
find was a “The
prospective study was carried out at the Academic Department of Surgery,
Consultation and Training Centre, Faculty of Medicine, Kuwait University
(Jabriya, Kuwait) in 83 obese subjects (39 men and 44 women).” [28]
The decline in the rate of weight
loss in this 24-week study indicates a lack of compliance, since the keto diet
avoids the effects of leptin at 8 weeks.
Other indicators are their triglyceride level which should have been
lower, as to the fasting glucose which leveled off at 5.65 mmol/L at week 16
through to the 24th week.
From week 8 it was as 5.8, at baseline it was 7.3 mmol/L. Compared
to the results of Margret, and
there are many other case examples and the well documented issue of compliance,
the ketogenic diet, short of starvation, is the most effective for those who
comply with the 5% carbohydrate limit and follow it by the 10%
maintenance.
The
science behind the weight loss finds 4 ways in which a KD improves weight loss
compared to CER.
The possible reasons for
the effectiveness of KD for weight loss may be listed as follows, in order of
evidence, strongest first:
- Appetite reduction:
protein satiety, effects on appetite-related hormones such as ghrelin, and
possibly a sort of direct appetite-blocking effect of KB
- Reduced lipogenesis and
increased fat oxidation
- A reduction in respiratory
quotient may indicate a greater metabolic efficiency in fat oxidation
A thermic effect of proteins and
[1] Antoni, Rona, Kelly Johnston, et al, March
2014, The
Effects of Intermittent Energy Restriction on Indices of Cardiometabolic Health
[2] Fothergill, Erin, Juen Guo, et al, May 2016, Persistent metabolic adaptation
6
years after “The Biggest Loser” competition
[3] A
though on the net result of losing significant weight as to caloric needs. Suppose
a 100 pounds of fat is lost. Since the adipose tissue use of ATP is quite
low—after all is an energy storage vault, it has a very low rate of metabolism,
compared to myocytes. Thus a person who
goes from 400 pounds to 300, shouldn’t all things being equal expect his
metabolism to drop by 25%, but a bit
less than 10% (I don’t know of on-point studies).
Thus Paul hasn’t with bariatric surgery has
stopped the WRS from lowering his metabolism to restore the lost weight.
[4]
Mind virus, coined by Richard Dawkins, for false beliefs that are passed around
like a virus.
[5] Plants
of the Gods, is a seminal work by two giants, Richard Evans Schultes
and Albert Hofmann, which was updated in new edition in 2001 by othes. Over
100 plants are listed with information
on their neuro-active chemicals.
[6] The
module description of the brain is used both in evolutionary psychology and in
neuroscience.
[7] Shi, Shu-qun, Tasneem Ansari, et al March 2013,
Circadian disruption leads to insulin resistance and obesity. They used
Bmal-1 knock-out mice to
demonstrate the mechanism. “Moreover, clock-disrupted Bmal1-knockout
mice are locked into the trough of insulin action and lack rhythmicity in
insulin action and activity patterns.”.
[8]
Okamura, Hitoshi, Shun Yamaguchi, et al, July 2002, Molecular machinery of circadian
clock in mammals
[9]
There are few rare exceptions where social conditioning (status) creates in a
select sub-population obesity; e.g.. the Suma wrestler
[10]
The Merck Manual, 8th Edition, 1950, p 266.
[11] The
fat switch, P 71.
[12]
Wiki, Urate oxidase, Dec 2019.
[13] Moss,
Michael, Salt sugar fat: how the food
giants hooked us, 2014. While
telling the history of food manufacturers function, we get a glimpse of profits
before people.
[14] Gardner, Christopher, Alexandre Kiazand, et
al, March 2007, JAMA, Comparison of the Atkins, Zone, Ornish,
and
LEARN Diets for Change in Weight and Related Risk Factors
Among Overweight Premenopausal Women
[15] Based on the production of pyruvate per calories,
there are about 1/3rd more calories per pyruvate from palmitic acid
compared to glucose; this is a rough approximation in a much more complex
process. I failed to find
an
article comparing per calorie or per gram the production of ATP.
[16]
Proteins were increased from baseline to 24% at 12 months, Supra P 973.
[17] Gardner, Christopher, Alexandre Kiazand, et al, March 2007, JAMA, Comparison of the Atkins, Zone,
Ornish,
and
LEARN Diets for Change in Weight and Related Risk Factors Among Overweight
Premenopausal Women
[18]
The LEARN isn’t a diet but rather based on lifestyle changes, and so data on
calories were not collected.
[19] Alhassan,
S, S. Kim et al, 2007, JAMA, Dietary
adherence and weight loss success among overweight women: results from the A TO
Z weight loss study
[20] Alhassan, S, S. Kim et al, 2007,
JAMA, Dietary adherence and weight loss
success among overweight women: results from the A TO Z weight loss study
[22]
The video by What I’ve Learned shows the cover of the article and the reference
page with its date, but just the quote of Williams in very large print and 2
food pictures below. I could not find after
over 30 minutes the article using Google.scholar and Medline.
[23]
This is a generalization which I find applicable in my own case, but younger,
fit, and overweight dieters probably have significantly different
experience. I
have not found studies done on the keto
flu.
[24]
Proteins are filling, and when measured by the net production of ATP, the 6
calories form a calorimeter is inaccurate. It is about 2.5 calories. Therefore,
the higher protein version of the
original Atkins diet is superior and it has a higher compliance.
[25]
The same would apply to statins, they should be taken at night slow release low
does. There are benefits for niacin,
which has many bio-functions, including lowering the mortality rate long term,
but for statins it is net harm.
[26] Paoli, Antonio, Antonio Blanco et al, July 2015,
The ketogenic diet and sports, a
possible marriage?
[27]
An inflammation of the gastrointestinal track (stomach and small intestine), for
which I prefer the older usage of it to include the large intestines and to
blanket the various inflammatory bowel conditions such as Crohn’s,
dirverticulitis, and others. Naming a
condition on symptom has a low rate of confirmation, and often the testing
falls well short of high percentage confirmation of diagnosis. Gastroenteritis
is a major cause of death mainly
in children of the 3rd world, about 700,00 yearly under the age of
5. About half of cases are in adults, with
increased risk because of poor sanitation, food handling, elderly, and among
those on a PPIs or polypharmacy. If the
condition persists over 3 weeks, I would take an enema and a strong laxative to
flush the system out and hopeful permit the normal bacterial flora to replace
the pockets toxin secreting bacteria or protozoa, or if invasive pathogen to
have those destroyed by the immune system.
Fasting can starve the pathogenic colony as to a ketogenic diet without
vegetables. Stressing the colony can help the immune system. If these fail,
the fecal enema has a high
cure rate. Unfortunately, the money
interest has continued their war against this drug free alternative, and
through guidelines have made this alternative unattractive to licensed care
givers.
[28] Dashti,
Hussein, Mathew Thazhumpal, et al Fall 2004, Long-term effects
of a
ketogenic diet in obese patients
6. How bariatric
surgery
causes permanent weight loss: Studies on the hormonal
changes following bariatric surgery is a window on why some avoid the
restoration of weight. Another study
showed that the increased fat was associated with t2d, and that following it
“drastically decreased.”[1] This confirms the work of Roy Taylor and team
at Newcastle University of the increase in pancreatic fat as causal for t2d.[2] Bariatric surgery, causes both a major
reduction in weight and it cures those most with t2d within 2 months, before
major weight loss (also covered in 6:4. 6). I have found just three
long-term follow up of bariatric surgery and a significant percentage keep
their weight off and many of the diabetics are off their drugs. The
results are superior for the Swedish study.
The 2 studies have a control group who weren’t operated on. (A
3rd study will be covered below
these two). These studies have mortality
figures and from them we must assume an improvement in quality of life over the
control group. In the 10.9 year follow
up of the Swedish study following 2010 with surgery and 2037 without surgery,
there was about a 25% increased survival with surgery, and at the 10.9 years a
19% reduction in weight. [3] Interestingly, of the deaths, there were 25
from MI in the control group and 13 in the surgery; but for cancer the
unexpected 47 and 29 respectively.[4] See 2 paragraphs below for my solution to the
anomaly.
In the study published in the NEJM, Sept 2017, which
had a 12-year follow up, there were 3 groups of severely obese, bariatric
surgery for which 418 had the Roux-en-Y bypass, second group of 417 who sought
surgery but for lack of insurance didn’t have surgery, and 321 who didn’t seek
surgery. During the 12-year follow-up
35% of the second group and 12% of the third had surgery. At 12 years for the 3
groups the adjust weight loss was 35 kg, 3 kg,[5]
and 0 kg respectively (these latter 2 groups included the 35% and 12% who
subsequent to baseline had bariatric surgery).
“Among the surgery group who had type 2 diabetes at baseline, type 2
diabetes remitted in 66 of 88 patients (75%) at 2 years, in 54 of 87 patients
(62%) at 6 years and in 43 of 84 patients (51%) at 12 years” [6]. Weight loss was, 45 kg, 36 kg, and 35 kg at
2, 6 and 12 years; thus a net 10 kg gained at 12 years, a 22% regain. Thus compared
to other studies using CER, the
difference is like night and day. It seems like
the hormonal changes that cured t2d also
occurred in those who weren’t diabetic.
This raises the question of what hormonal changes relevant to resting
the WRS occurred Roux-en-Y surgery group (#12).
The drop in the number of patients in the follow-up
of the surgery group was because of suicide, “5 patients of the gastric-bypass
group died by suicide” Supra. None of the other 2 groups who didn’t have
surgery committed suicide. Note, 2 of
the 2nd group who had the surgery committed suicide. The author goes
on to say that the suicide
and self-harm “have been shown by previous studies” (supra).
Unlike the author, who probably isn’t aware
of the
association of neuroleptic drugs with self-harm, I hold that it is the cause (4:5). Those who undergone surgery are more likely
to be given neuroleptic drugs (drugs that cause drowsiness other than opioids)
and this is strongly associated with suicide, weight gain, and polypharmacy. Those who had the operation are likely to be
put on a sedative in the hospital and continued thereafter. Neuroleptics are a
gate way drug inhibiting cognitive function and thereby increasing their
reliance up their pill-pushing physicians.
Confirmation of my hypothesis on neuroleptic drugs as slow poison and a
strong association with polypharmacy will require the opening of the data
banks.
The Swedish study for which the cancer rate increased
from 29 without surgery to 47 with surgery.
The increase in cancer I hold would follow from polypharmacy, especially
the reduction in metabolism caused by neuroleptic drugs. The US study didn’t
track deaths from
cancer. Like with statins and dementia,
pharma funds studies that deflect this obvious consequence by pharma’s studies
finding a reduction. We won’t know the
numbers of deaths associated with drugs until the data banks are open for real
world population studies.
As for the mechanism for weight loss, the Roux-en-Y is very significantly better than
the gastric band (#8) for its curing t2d. BMI at 2 years was 29.7 compared to 36.3 for
the band. The hormonal cause was
measured:
Likewise, leptin levels were lower in the patients who
underwent Roux-en-Y (P = .003), and levels
correlated with weight loss, loss of fat mass, insulin levels, and Homeostasis
Model of Assessment 2. Adiponectin correlated with insulin levels and
Homeostasis Model of Assessment 2 (r = −0.653, P = .04
and r = −0.674,
P = .032,
respectively) in
the patients who underwent Roux-en-Y at 24 months.[7]
However,
with insurance companies deciding the treatment, the much less expensive
gastric band is the standard or similar less invasive treatment dominates.[8] Dollars before patients.
Others studies support the conclusion that
biliopancreatic diversion group has the best result. In a 2012 study 75% with
gastric-bypass and
95% with biliopancreatic diversion at 2 years were still in remission, and as
expected a lower glycated hemoglobin level, 7.69 for the standard treatment
gastric bypass group compared to 4.95 for the biliopancreatic group.[9]
This clearly is a sign of regulatory hormonal changes (#12)
It has been proposed by Jason Fung and others that
a
type of fasting occurs following surgery, when the person is fed intravenously
a low calorie infusion. Fung et al hold
during this period there is significant improvement in the diabetic
patients. This improvement occurs before
significant weight loss, which is pharma’s explanation. Fasting has been
proposed by Jason Fung and
others. Through the extended fast it has
been proposed that the fat in the excess lipid droplets in liver and pancreas
have been metabolized, ant this changes results in a reversal of IR and
restoring the WRS, and with that a major improvement in homeostasis. More studies are
needed to confirm these changes, thus showing what is causing the reversal of
IR. Something has happened to
avoid the yo-yo diet, something that distinguishes them from the biggest losers
that has caused a reversal of IR.
7. Going without food--fasting: In a lecture
by Dr. Jason Fung relates his 6-year old son’s reply
to the question, how do you lose weight?
“Simply, don’t eat!” There are
two well established ways to lose weight, one is to turn up the daily rate of
fat metabolism by lowering glucose metabolism, the other is by fasting, which
of course turns up fat metabolism. Both
have many variations as to methods.
Since the two are complimentary, it would seem that the combination of
both is superior to just one of them; and it is! Now to resolve, what fasting
type is best for
one’s situation?
Medicinal
fasting, historical background: Before there was bariatric surgery, water fasting
was
the most successful treatment for the morbidly obese and obese. The patient
was monitored in a metabolic ward
of a hospital, or as an out patients.
For most, health issues were minor, because like other mammals we have
evolved to go long periods without food.
A normal weight male during starvation can go over 4 weeks before
metabolizing muscle during starvation—autophagy of skin and adipose tissue
supplies needed amino acids for autophagy.
The fit, thin male is about 13% fat, while the fit woman is about
23%. At about 7% for men the body adds
from fat metabolism to amino acids from muscles to also contribute to the ATP
production. A normal weight (thin) woman
has near twice the store fat and takes longer before they metabolize
muscle. Biological like other mammals we
are designed to survive prolonged food shortages—most common being
underfed. Since being underfed would
include some carbs, the adaptations would be different, one of which is hunger
being greater. However, when the stored
fat is quite low (~ 7%) the body switches into another phase to conserve fat
through diminished ATP for movement, and to metabolize muscle so as to conserve
fat. Note fat is essential for building
cell membranes for repair and replacement, thus the reserve is mainly for that
purpose and as a building block for other bioactive molecules.
PHASES OF STARVATION In the
transition from the fed to the fasted
state, a sequence of metabolic alterations occurs, listed as follows with their
approximate duration: 1) Gastrointestinal absorption of substrate 1-6 hours 2)
Glycogenolysis 1-2 days 3) Gluconeogenesis first week 4) Ketosis 3-4 days
onward 5) Diminishing gluconeogenesis and increasing cerebral ketone
consumption second week onward/[10]
Five biological changes occur during
starvation; they were identified in the 1970s George Cahill Senior, Harvard
Professor. In the earlier stages there
is an increase the level of the catechol amines and human growth hormone (HGH)
which in turn stimulates IGF-1. IGF-1
stimulates serum glucose and FFAs. The
net result from the catechol amines and maintenance of the energy molecules
more energy and mental alertness—a survival advantage. Later stages operate
to produce glucose for
erythrocytes[11]. This is at the reason why those who try
alternate fasting and extended water fasting report that they feel fine. Moreover,
measurements of leptin show that as
meals are missed its secretion declines and thereby the hunger.
Fasting has been used to starve cancer, because all
cancers have defective mitochondria; defective because apoptosis is initiated
by the MTD, and disabled MTD by past this mechanism for dismantling
significantly abnormal cells, the Warburg effect (3:3,
2). Three of my friends through
extended water
fast were cured of their cancers.[12]
There are a number of variation as to
what counts as a fast. For the sake of
discussion, and consistent with the journal literature, I adhere to the
standard of 600 calories a day for men and 500 for women, which has been used
for over a century, more calories will be labeled as CER.[13]
Currently, Dr. Michael Mosely has made that fast popular with his best-seller
books.[14] Whether the water fast is superior when used
for weight loss and for t2d, I cannot say; there are reasons for both.
Intermittent fasting: this
consists of going from three meals a day to one are two. Just missing one meal
in a study show an
average reduction in calories of over 500 per day. On top of that the duration
of fat metabolism
increase. Building upon that snacks
should be low in total digestible carbs, so as not to shut down fat metabolism
and autophagy. Meals too should be low
in carbs. I skip breakfast since 2014 6
days a week. I find it easy, and since I
am not on a weight loss program, I could do better at least twice a week by
skipping dinner. I also a couple of day
a month do a 22 hour fast, as I am in the medical library, and on those days I
take the snacks out of the car. Turning
up autophagy is healthy, thus everyone would benefit from intermittent fasting
who has been on the western diet.
Key points, assuming intermittent
fasting is for weight loss and thus better health. skip one meal a day is a
good starting point,
which can be extended. Low carbs improve
the results.
Find a sustainable pattern.
Alternate day fasting: This
is the next step up and should be used if the progress slows or stops with
intermittent fasting. It is simple, made easier once adjust to the intermittent
fasting, to switch to alternate day fasting.
Again by keeping the carbs to under 25% of calories on non-fasting day
the results improve.
As mentioned before, Michael Mosley’s 5:2 diet
has
been tried with success by millions, and his book was on the a #1 best seller
on the international non-fiction list. On the fasting days, calories are
limited to 500 for women and 600 for men.
There are many variations to this diet, many health benefits.
Extended water fasting, this has
the most healthful consequence, and one I
do at least once a year for 5 to 6 days.
Since I am at the normal weight I go strict ketogenic with about 500
calories a day from butter and cheese. I
do this because at the age of 76 (2019), I have what runners call hitting the wall. This hitting the wall didn’t occur until
about the age of 70. It is an extreme
lack of energy, for example, walking slow around the block or 20 minutes of
house cleaning is followed by exhaustion lasting several hours. Sometimes it occurs
without physical activity and there is a prior warning at least proceeding it
by a half hour that I need to eat and it must include some carbohydrates. This
might not occur for younger and heavier with extended water fasting.
As
repeatedly stated, the hormonal processes are what causes
weight gain, and the processes must be reversed for long-term weight loss: the
WRS establishes the level of fat; it must
be reset. “Adipose tissue functions not only as an important
buffer for fatty acids but also as a highly active secretory organ, capable of
influencing whole-body physiology through the production of an array of
bioactive Adipokines.” [15] The role of insulin in weight gain is beyond questioning both
at
the laboratory level and observational level.
The success of fasting is beyond questioning, and the combination of
high fat thus low carb diet with fasting entails the Randle cycle stays in the
fat metabolizing setting. There is a lack of quality long-term
studies of low carbs, of fasting, and the combination of the two. Studies are
need which measure, the effects
on liver metabolism, insulin and leptin levels, CER diets, and whatever else
would elucidate the processes.
Fasting also turns up autophagy
and thus
goes far beyond curing t2d:
There is large empirical
and observational evidence that medically supervised modified fasting (fasting
cure, 200-500 kcal nutritional intake per day) with periods of 7-21 days is
efficacious in the treatment of rheumatic diseases, chronic pain syndromes,
hypertension, and metabolic syndrome. The beneficial effects of fasting
followed by vegetarian diet in rheumatoid arthritis are confirmed by randomized
controlled trials. Further beneficial effects of fasting are supported by
observational data and abundant evidence from experimental research which found
caloric restriction and intermittent fasting being associated with deceleration
or prevention of most chronic degenerative and chronic inflammatory diseases.
Intermittent fasting may also be useful as an accompanying treatment during
chemotherapy of cancer. . . . Various identified
mechanisms of fasting point to its potential health-promoting effects, e.g.,
fasting-induced neuroendocrine activation and hormetic stress response,
increased production of neurotrophic factors, reduced mitochondrial oxidative
stress, general decrease of signals associated with aging, and promotion of
autophagy.[16]
Fasting is easier
than caloric restriction. It is easier
to stay out of the kitchen, to be away from food, than to be around it and
limit the portions:
Persistent hunger and irritability
noted in non-obese men and women in
earlier IER trials, where food was completely restricted on alternate days,
suggest that some individuals are unlikely to be able to comply for extended
periods of time. Compliance with IER
[intermittent fasting] protocols which allow some
intake on restricted days have been promisingly high. . . Findings from rodent trials suggest that IER (50-100%
ER/alternate days) is capable of modulating adipose physiology, independently
of changes to fat-mass. [17] [IER alternate days is alternate day
fasting, ER energy restriction, the 50-100%
is the amount of restriction of
rat chow on fasting days.]
The first part above is evidence that intermittent
fasting compliance is higher than CER. This is consistent with my observation
The second section quoted above states that through IER (alternate day fasting)
the adipose tissue hormones don’t kick in, in particular leptin, to cause
increased hunger and lower metabolism, a metabolic response to preserve adipose
tissue and restore its fat to prior level.[18] Thus alternate day fasting or the short
intermittent version are a way to lose weight, cure or manage without drugs
t2d, and avoid the at 2 months reduction in metabolism and increase in appetite
caused by leptin.
The benefit of IER
is improved insulin response. The
article points out that with moderate to high carb diet does the glucose level
rise to abnormal levels, and thus with low carbs the production of insulin is
sufficient to keep the serum glucose at a normal level. Clearly the low carb
diet is the way to
manage t2d.
Hepatic IR ensues, increasing
endogenous glucose production, hence
elevating plasma glucose levels and stimulating further insulin secretion. Within
pancreatic β cells, excessive lipid
deposition causes the metabolic inhibition of postprandial insulin secretion
which, above an individual threshold, will herald the onset of hyperglycaemia. Within
pancreatic β cells, excessive lipid
deposition causes the metabolic inhibition of postprandial insulin secretion
which, above an individual threshold, will herald the onset of hyperglycaemia.[19]
It
isn’t rocket science that the low carb diet is the way to keep serum glucose
within the normal level and thus not need drugs for managing it, and IER is the
most effective of the many types of diet for significant weight loss.
This brings back to
what I would do if my BMI was above 30.
I would do a long-term water fast, and if that proved difficult, I would
include small snack low in carbs and high in protein, and if I feel I need more
energy add butter. I would add to that
male hormone replacement, and for women estradiol with progesterone for seniors
(6:2) because of
their role in lipodystrophy and metabolism.
I would also take three-325 uncoated aspirin[20]
because it lowers blood glucose and has been used in very high dose to cure t2d
(see http://healthfully.org/rc/id3.html under diabetes heading). The object is to reverse insulin resistance
and
improve quality of life.
For lower risk
for
CAWD: Risks for an assortment of conditions has in the literature
been
shown to be lowered by extended fasting:
There is large empirical and
observational evidence that medically
supervised modified fasting (fasting cure, 200-500 kcal nutritional intake per
day) with periods of 7-21 days is efficacious in the treatment of rheumatic
diseases, chronic pain syndromes, hypertension, and metabolic syndrome. . . .
Further beneficial effects of fasting are supported by observational data and
abundant evidence from experimental research which found caloric restriction
and intermittent fasting being associated with deceleration or prevention of
most chronic degenerative and chronic inflammatory diseases. . . . Various identified
mechanisms of
fasting point to its potential health-promoting effects, e.g., fasting-induced
neuroendocrine activation and hormetic stress response, increased production of
neurotrophic factors, reduced
mitochondrial oxidative stress, general decrease of signals associated with
aging, and promotion of autophagy.[21]
Autophagy is what reverses IR and t2d by metabolizing
lipid
droplets that cause pancreatic inflammation and its beta cell dysfunction. Autophagy
selective follow the surgery
promotes the metabolism of pancreatic lipid droplets and hepatocytes
droplets.
8. Extended
water fast, Angus
Barbieri:

An example carefully tracked by physicians and in
the
Guinness
Book of Records is Angus Barbieri, a 456 lbs. record water fast. Angus
is Scotsman from Tayport. “Initially
there was no intention of making his fast a protracted one, but since he
adapted so well and was eager to reach his “ideal” weight, his fast was
continued into what is presently the longest recorded fast (Guinness Book of Records, 1971).” [22] Starting
in June 1965, at the age of 27, he went on a medically supervised water fast
lasting 382 days and lost 276 lbs. to obtain his goal of 180 lbs. He consumed
only vitamins (Paladac), vitamin
C, yeast, electrolytes, and zero-calorie beverages. Initially he was treated
in the hospital,
“but for the greater part of the time he was allowed home, attending regularly
as an out-patient for check-up” (supra).
Monitoring for health reason would reveal any
significant consumption of food.
“Twenty-four hour urine collections were made periodically throughout
the fast. His mean urinary creatinine
excretion was 1541 mg/24hrs, with a deviation of 25% from the average. . .
there were 37-48 days between stools latterly.” (supra). His fortnight
blood test included tolbutamid
(sulfonylurea drug), glucose tolerance, and glucagon tests, as tests for
carbohydrate metabolism. Tolbutamide was
given 1 ½ hours after glucose infusion.
“Test for glucose tolerance showed unimpaired capacity for glucose
uptake” [IR cured] (supra). His average blood glucose was 30 mg/dL (1.7
mmol/L),[23]
which confirmed that he wasn’t eating carbs—as too his weight loss. The
low level of glucose is consistent with
others studies of long-term water fasting.[24] He was well below what causes hypoglycemia
shock in diabetics 40 mg/dL, (2.2 mmol/L).
Hypoglycemia in diabetics is listed at 70 mg/dL (3.9 mmol/L). The sudden
drop of glucose of diabetics,
without the 5 metabolic shits that occurs over a period of about 5 days, this
is the reason for diabetic hypoglycemic shock.
The case study was published 7 years later. He didn’t need an operation to remove the
skin folds because autophagy metabolized the excess skin and adipocytes to
supply the needed amino acids for autographic cellular repairs—the recycling of
amino acids. Only when fat stores become
low, then the body starts metabolizing muscle—that occurs when fat drops below
7%. On his examination at 7 years, Angus
had gained only 16 pounds—much better than the contestants
on The
Biggest Losers show.[25] Note:
after an hour, I gave up on trying to find Angus’s
cause of death at the age of 51 and weight at that age.
Not all are so fortunate, and a friend of mine, a
middle-age geriatric physician, had to undergo surgery to remove his
folds. I recall him power walking around
the track holding the large flaps of skin with subcutaneous fat on each side
against his body. He lost nearly 150
pounds eating 1 meal a day for a year.
With the social support of his wife, a nurse, he kept the weight off, an
indication that his insulin resistance was reversed and with a supportive
social environment he did not at 5 years become obese again.
9. Amino acid and insulin: It
is widely circulated that certain amino acids raise inulin; the combination of
essential amino acids raise insulin the most.
It is a topic I have been pondering over since 2015. Why should insulin
go up when amino acids
increase in the blood? I stopped nibble
on cheese during my intermittent fast in the morning in 2016. In 2018, I found
an article which stated that
it only happened when consuming proteins with carbs. So I started again cheese
nibbling. Then in December of 2019 I searched insulin amino acids and fond that the
glucose amino acid combo was wrong, that the essential amino acids (30 grams
infusion) would cause for 1 hour an insulin spike significantly greater than
any one of the amino acids.[26] The spike of the 30 was similar to an
infusion by glucose. So why has nature
given us an insulin spike for essential amino acids.
Nature is very good at fine-tuning
processes on a cellular-molecular level.
In general, the more significant for survival and reproduction the finer
the adjustment are and the more complex the processes. For example the adipokines
(also known as
adipocytokines) are cell signaling proteins secreted by the adipose tissue: “The first adipokine to be
discovered was leptin in 1994.[1]
Since that time, hundreds of adipokines have been discovered.”[27]
I bring adipokine to give an idea of the complexity of the homeostasis
systems and by extension that it is very likely there
is a system that responds to amino
acids and doesn’t lower blood glucose is both possible and likely.
That the essential entails
stimulate insulin and doesn’t respond to the non-essential amino acids which
are synthesized as needed, this suggests that the insulin has another function
besides stimulating glycogen synthesis, the release of glucose by the liver,
and the uptake by cells of glucose.
Insulin also stimulates the product and release of two androgens, IGF1
and IGF-2—insulin like growth factors.
The insulin rise is because of the need to utilize the amino acids which
can’t be stored. The growth factors
stimulate skeletal muscle and other targeted tissues growth. Thus insulin is
signalling for the synthesis
of proteins as needed. I suspect that this
doesn’t throw the Randle cycle into glucose metabolism unless there is
significant amount of carbs—not a common occurrence among paleo peoples who
tended to eat only one type of food at a meal.
The modest
drop in serum FFA during the insulin spike caused by amino acids suggest that
fat metabolism continues and their conversion into triglycerides.
Another piece of the puzzle is the
in mammals glutamine is part of the mTOR, regulation system and this turns on
autophagy by down regulation of mTOR.[28] Liver autophagy not only promotes both the
anabolism and catabolism of the amino acids during fasting, but also the
regulation of blood glucose.[29] Whatever the details the net purpose of
autophagy and insulin is to increase survival in the natural environment.
Unlike the affluent populations,
paleo peoples didn’t make a ritual out of meals, but for special
occasions. They didn’t eat a balance
meal, but rather often ate just one food.
Thus they would eat meat without starches, or starches such as taro
without meat, or just nuts; etc.
Secondly scarcity of meat and other protein sources in some populations
supports a set of thrifty genes for the construction of proteins, and such
construction requires autophagy thus the role of insulin is different when the
carbs are low in a high protein meal.
As for my diet, I am still doing
the intermittent fast, and since I am at my ideal weight, I am not on a weight
reduction program. The last time I was
in 2003, when after 2 weeks with relatives, I put on 15 pounds, which I
promptly took off when returning to California.
Since then with the supplement of testosterone high dose from a
compounding pharmacy, I have not attempted to lose weight. I naturally stay
within the around 160
lbs. The WCS is working as
designed. Prior to that since I was 27,
I would watch my weight, and when it creeped up 6 pounds I would cut back on
portions. I believe that the
testosterone makes a major difference, and that I was on two 325 mgs of aspirin
daily—aspirin lowers serum glucose.
With my current diet my snacks are
small portions of cheese, about 8 grams with about 12 grams of butter, or I eat
bell pepper with homemade Russian dressing.
Small portions low in carbs keeps my insulin low and I stay in mainly
the fat metabolizing mode. I have come
to believe based on a number of trials with alternate day fasting and calories
up to 500 per day women and 600 men that the results aren’t compromised and the
compliance is significant.[30] The complexity has
promotes efficiency,[31] thus I presume on
indirect evidence that proteins with fats in moderate amounts do not overturn
the apple cart, that they are an ideal snack in addition or with leafy
vegetables.
Dietary examples support this
conclusion that proteins don’t cause fat storage. The success of the high
protein low carb
diets stands as evidence. The Banting
diet[32] and that of Atkins
have both done better than the low carb
CER diets.
I mention this about proteins so
that those who wish to try out intermittent fasting, high fat diet or alternate
day fasting will have some tips by one who is strong in nutritional science and
practical experience. The evidence supporting both long-term water fasting, and
also low carb fasting comes from many directions. If your body sends a strong
message to eat, try as I do, the protein saturated fat snacks. Remember that
are appetite is set up to
promote survival as long as it is properly functioning as it does for the
LSPs.
Wasting t1d prior
insulin days: given
what has been said of the role of
insulin as to its regulatory function for the insulin like growth factors.
10. A modern update on diet: What diet depends
upon one’s health, for
which I have broken down into 5 diets depending on situation, at http://healthfully.org/rh/id8.html.
Empower the rational module of the brain by watching the YouTube videos
listed at http://healthfully.org/rh/id7.html under categories 1, 2 and 3—knowledge
effects behavior. If I was
diabetic. We are a social animal, thus
for most people it is necessary to get the support of the significant
other. Having them watch the videos is a
start. Work on them to be supportive by
using condition techniques of reward and withholding rewards. It is hard to
diet when the other half is an obstacle.
If I was overweight
or worse, I would start with low sugar and intermittent fasting while gradually
lowering carbs and increasing saturated fats.
I wouldn’t count calories. When
not hungry skip a second meal. Non-carb
snacks help. I snack on cheese with a
big wad of butter (zero carbs), sometimes it is salted nuts with butter. Sex
hormones (6:2) play an important role. I am 76 as of 6/19, have been on this diet
since 2014 with intermittent fasting since 2014 and low sugar. Lower carbs was
introduced in 2016. However, I have always been of normal weight
so I don’t try to lose more weight. I
haven’t watched my weight since I started testosterone replacement in
2003.
If I had t2d I would go on a very
low
carb, high fat diet with extended water fasting to metabolize the lipid droplets
in the liver and pancreas. Once
restoring weight and glucose metabolism to normal, I would stay on a high fat
diet with intermittent fasting (#5). I would once ideal
weight increase carbs to about what is craved.
I currently get about 20% of ATP from carbs 70% from fats and 10% from
excess amino acid. Let the body be the
guide, unless the leptin system is causing weight gain. Intermittent fasting
might be sufficient,
otherwise continue with alternate day fasting and lowering carbs. There would
be no need to say no to the drugs?
Water fasting or if too difficult
extremely low net carbs[33]
is a key part of the cure. The fast
increases autophagy with a major increase in mitophagy. The rate of replacement of the MTD in the liver peaks at 1.25 days; the control
at 1.85 days, and there is nearly zero overlap of the 2 bell curves.[34] The article goes on to warn that using
fasting glucose and BA1c are inferior to that of “changes in circulating
insulin concentration, fasting (hepatic) insulin sensitivity, and glucose
uptake/clearance. ..”[35]
The mitophagy increase is the key part of what gives the superior results. Moreover,
in this seminal review article it
noted with references to 6 articles that “Compliance with IER [intermittent
fasting] protocols which allow some intake on restricted days have been
promisingly high” (supra). The review article supports both dietary
management of
t2d but also through fasting with low carb its cure.
11. Ketogenic diet

Much of what has been said about multiple day water fasting
applies to the ketogenic diet in that both, both metabolize fat
producing ketone bodies, both turn up autophagy, both cause significant weight
loss, both improve insulin sensitivity, and both have been shown to treat or
reduce the risk of a number of conditi Much
of what has been said about the salubrious effects of fasting can be said of a
ketogenic diet.
D-beta-hydroxybutyrate, the principal "ketone" body in
starving man, displaces glucose as the predominating fuel for brain, decreasing
the need for glucose synthesis in liver (and kidney) and accordingly spares its
precursor, muscle-derived amino acids. Thus normal 70 kg. man survives 2-3
months of starvation instead of several weeks, and obese man many months to
over a year. Without this metabolic adaptation, H. sapiens could not have
evolved such a large brain. Recent studies have shown that
D-beta-hydroxybutyrate, the principal "ketone", is not just a fuel,
but a "superfuel" more efficiently producing ATP energy than glucose
or fatty acid. In a perfused rat heart preparation, it increased contractility
and decreased oxygen consumption. It has also protected neuronal cells in
tissue culture against exposure to toxins associated with Alzheimer's or
Parkinson's. . . . Efforts are underway to
prepare esters of beta-hydroxybutyrate which can be taken orally or
parenterally to study its potential therapeutic applications.[36]
Beta-hydroxybutyrate
stimulates neurotropic factors, for which there is evidence that it slows the
progression of Alzheimer’s disease, and has been used to reduce to block
epileptic seizures since 1920, and guidelines recommended for intractable cases
for children, after the sedatives have proven unsatisfactory—thankyou pharma for the limits. “In
a
retrospective chart review of patients who had been on the diet for 6 years, 24
out of 28 patients had experienced more than a 90% reduction in seizures.” [37]
As an adult which would you do if having
frequent seizures. One of my neighbors
is constantly low (not high) from the same treatment for intractable
migraines. Yes, there is evidence in
support of treating migraines with a ketogenic diet—and also for dementia.
Why carbohydrates are fattening
unlike fats: Insulin through the overstuffing of cells
with glucose causes two things that promote weight gain when the WRS points to
the right. One is by synthesis of fats,
the other by conversion of fatty acids into the storage from of triglycerides
by the addition of glycerol.


Acetyl–CoA
Pyruvic
acid--pyruvate is the base
Acetyl-CoA (acetyl coenzyme A) is a molecule that
participates in many biochemical reactions of protein, carbohydrate and lipids metabolism.
Its main function is to deliver the acetyl group to the Krebs cycle to be oxidized
for energy production. Two Acetyl-CoA
through several steps gives rise to acetoacetate, beta-hydroxybutyrate and
their break down product acetone, which are called ketone bodies. They are mainly
produced by the liver and
released into the blood. All cells with
mitochondria (that includes all cells in the nervous system) can take up the
ketone bodies. Acetyl CoA can also be
used in the cytosol to form fatty acids or converted to malonyl CoA for the
synthesis of fatty acids. Acetyl CoA can
also enter the melavonate pathway which makes several essential compounds
including cholesterol. Acetyl is a
substrate for flavonoids, polyketides, steroids, phospholipids, and on and
on.
Pyruvic acid is made from glucose and enters
the Krebs cycle when
oxygen is present; when not it is metabolized in the cytosol in a process
called fermentation.
A more detailed explanation of
the
synthesis of fats from carbohydrates: when insulin is high due to blood glucose,
the cells become stuffed with glucose.
When there is sufficient ATP a feedback system causes the use the citrate
(produced by the condensation of acetyl CoA with oxaloacetate) in the Krebs
cycle. This turns off the production of
ATP temporarily. When the level of ATP
is sufficient the acetyl CoA is carried across the inner mitochondrial membrane
into the cytosol. In humans, fatty acids are formed from
carbohydrates predominantly in the liver and adipose tissue, as well as in the mammary
glands during lactation. The pyruvate (pyruvic
acid) produced by glycolysis is an important intermediary in the conversion of
carbohydrates into fatty acids and cholesterol.
Most
of the acetyl-CoA which is converted into fatty acids is derived from carbohydrates
via the glycolytic
pathway.
12.
A listing of what is best for dieting for weight loss, managing
diabetes, and lowering risk for CAWD (in approximate order of importance):
SOCIAL FACTORS: building
the will power to behave differently
Enlist
support of roommate, significant other,
friends, family, and others Watch
daily the documentary and lectures at http://healthfully.org//rh/id7.html ON
DIETING:
Intermittent fasting Extended
low carb fasting Alternate day fasting[38] Very
low digestible carb snacks[39] Ratio
of fats 75% to carbs 25% in calories (not counting proteins) Hormone
replacement after the age of 60 men 50 women (6:2) On
non-fasting days no digestible carbs 3 hours before going to sleep Strenuous
work or exercise including weight training—especially if on HRT
[1] Gaborit, B, I Abdesselam, et al, July 2014,
Ectopic
fat storage in the pancreas using 1H-MRS: importance of diabetic
status and modulation with bariatric surgery-induced weight loss
[2] Knop, Flip, Roy Taylor, August 2013, Mechanism of Metabolic Advantages After
Bariatric Surgery: It’s all gastrointestinal factors versus it’s
all food restriction. Prof. Roy
Taylor has several lectures on YouTube on this topic.
[3] Sjostrom,
Lars, Kristina Narbo, et al Aug 2007, Effects of Bariatric Surgery on
Mortality in Swedish Obese Subjects, FULL, while suicides are not listed,
sudden deaths are 20 vs 14 for the non-surgery.
This greater sudden death rate
probably reflects the reluctance in reporting suicide, and the requirement for
clear evidence that it was suicide as cause of death.
[4]
Unexpected because there is a strong association of cancer with obesity, thus
the surgery group should have had less caners.
[5]
Many of them had the surgery years later, and many would have had a type
surgery which reduces the size of the stomach, for which the evidence on
benefits are well below that of the Roux-en-Y type of bypass.
[7]
Trakntenbroit, Michael, Joshua Leichman, et al May 2009, Body Weight, Insulin Resistance,
and Serum
Adipokine Levels 2 Years after 2 Types of Bariatric Surgery. In another study at 12 months
the BMI was also 29 for the Reux-en-Y bypass, Polyzogopoulou,
Eftihia, Fotios Kalfarentzos, et al, May 2003, Restoration of Euglycemia and
Normal Acute
Insulin Response to Glucose in Obese Subjects With Type 2 Diabetes Following
Bariatric Surgery, and their t2d was cured at 2 months.
[8] Pareek, Manan, Philip
Schauer, et al Feb 2918, Metabolic
surgery: weight loss, diabetes and
beyond
[9] Mingrone,
Geltrude, Simona Panunzi, et al April, 2002, Bariatric
Surgery versus Conventional Medical Therapy for Type 2 Diabetes
[10] Cahill
Georg F Jr., May 1977, Physiology of
acute starvation in man
[11] I have
failed to find evidence that certain cells in the brain need glucose, since the
measurement aren’t sufficiently selective to exclude erythrocyte glucose
metabolism.
[12] All cells
require a supply of ATP, the more metabolically active the more ATP. In most
the MTD have been sufficiently disable
so that dep[end totally on the cytosol for the production of ATP through a
process called fermentation, fermentation of glucose. A diet lack glucose will
starve the cell,
since the alternate glutamate isn’t in sufficient amount to yield enough ATP
for cancer cell maintenance. Ethics
committees for approving clinical trials have block the clinical trials using
just water fasting, or they require chemotherapy first. But the fully functional
immune system is need
to destroy cancerous cell, and chemo very significantly weakens the immune
system.
[13] Tsukahara,
Satooru, Makoto Ohno, et al, 1988, (book), Diet
and Obesity p. 205-227, Dieting using a very low calorie diet
[14]
Unfortunately, he doesn’t limit carbs for the obese, but does for diabetic and
prediabetic, and recommends a high fat diet to replace the carbohydrates, The
8-week blood sugar diet: how to beat
diabetes fast (and stay off medication) P 67-9 & elsewhere.
[15] Antoni, Rona, Kelly Johnston, et al, March 2014, The
Effects of Intermittent Energy Restriction on Indices of Cardiometabolic Health
[16] Michalsen A, C
Li, Dec 2013, Fasting Therapy for Treating and Preventing Disease - Current
State of Evidence
[17] Antoni, Rona, Kelly Johnston, et al, March 2014, The
Effects of Intermittent Energy Restriction on Indices of Cardiometabolic Health
[18] Antoni, Rona, Kelly Johnston, et al, March 2014, The
Effects of Intermittent Energy Restriction on Indices of Cardiometabolic Health
[19] Antoni, Rona, Kelly Johnston, et al, March 2014, The
Effects of Intermittent Energy Restriction on Indices of Cardiometabolic Health
[20]
The coated aspirin takes 5 hours on an empty stomach and 8 hours on a full
stomach to reach peak blood level, and total aspirin absorbed is one half that
of the uncoated aspirin—part of bad pharma’s assault upon aspirin.
[21] Michalsen
A, C Li, Dec 2013, Fasting Therapy for
Treating and Preventing Disease - Current State of Evidence. Last 3 words
shouldn’t be promotion of autophagy bur rather one
facet, promotion of apoptosis.
[22] A
case study was published 7 years later, Stewart, William, Laura Fleming,
March 1973, Features of a successful therapeutic
fast of 382 days' duration
[23]
This level is well below that which causes symptomatic hypoglycemia and
death. During extended fasting the liver
adjusts to the lack of food by producing glucose, and other adjustments
occur. Medical supervised water fasting
was used to reverse obesity prior to bariatric surgery. Drenick, Ernst, Marion, Swendseid, et
al Jan, 1964, Prolonged Starvation as Treatment for Severe Obesity
[24]
The diabetic coma from hypoglycemia is caused by a failure of the body to make
metabolic adjustments to the rapid change in serum glucose. There are 5 metabolic
switches that occur
with extended water fasting.
[25] See
Jason Fung, The complete guide to fasting,
2016, P 104-106, who relied upon
the New York Time’s article mostly, which was based upon an article in Obesity,
Fothergill, Erin,
Juen Guo, et al, May 2016, Persistent metabolic adaptation 6
years after “The Biggest Loser” competition.
[26] Floyd, John, Stefan Fajans, et al, sept 1966, Stimulation
of insulin secretion by amino acids
[27]
Wiki Adipokine Jan 2020
[28] Nicklin,
Paul, Philip Bergman and 15 others, Feb 2009, Bidirectional Transport of Amino Acids
Regulates mTOR and Autophagy
[29] Ezaki,
Junji, Naomi Matsumoto, et al, Autophagy Vol. 7, 2011, Liver
autophagy contributes to the maintenance of blood glucose and amino acid levels
[30]
One well received case is that of Michael Mosley, whose 5- 2 diet book made it
to the best seller list: The
8-week blood sugar diet: how to beat
diabetes fast (and sty off medications and The fast die t#1 New
York Times Bestseller. His documentary
and interviews on YouTube are very good.
[31] Patti, ME, Brambilla, et al, April 1998,
Bidirectional modulation of insulin action by amino acids
[32] William
Banting, Letter
on Corpulence (1869) which is still in print a 150 years later.
[33] Net
carbs are total carbs minus the fiber.
A tern used by the group of professors that runs the New Atkins
diet.
[35] Antoni, Rona, Kelly Johnston, et al, March 2014, The
Effects of Intermittent Energy Restriction on Indices of Cardiometabolic Health
[36] [36] Cahill, George Jr.,
Richard Veech, Trans American Climatol Association, 2003, Ketoacids? Good medicine?
Beta-hydroxybutyrate is derived from
short-chain fatty acids. GF Cahill (1927
to 2012) research director of the Joslin Diabetes Center from 1962 to 1978. In
1970 he became a Harvard School of
Medicine professor. He was a leading
researcher on metabolism,
diabetes, fasting and related topics, number over 100 articles from 1958 to
1983, 25 years
[37] McArtney,
Rowena, Alexancer Bailey, et al BMJ, 2017, What is a ketogenic diet and how does it affect the use of
medicines?
[38]
Both #s 2 & 3 a limited numbers of calories, 500 for elderly and women, 600
for men with very low carbs will not significantly tak the dieter out of fat
metabolism through elevated insulin to cause conversion of free fatty acids to
triglycerides or shut down autophagy
[39]
This would consist of cheese, meets, fish, oils, green –leafy vegetables, nuts,
in small portions so as not to significantly raise insulin and thereby shut
down autophagy and causes the conversion of free fatty acids to triglycerides. These
types of snacks should be used to
extend diet and make repeating of 1, 2, and 3 more likely.
13. A personal note on how I ate the western diet
and escaped:
A number of socially driven behavior helped
me. First, my education and acceptance
of Greek wisdom, which held that the highest pleasures are intellectual because
of their duration and lack of negative consequences (if one had the spirit of
the Greek philosopher, which among other things stressed public spirit and
doing good). I was a philosophy major
with 2 years of graduate school. Second,
in 1974 on moving to California I notice that the fit and athletic were a
happier lot of people. So I socialized
with them and took up volley ball and cycling.
That help me metabolize sufficient excess sugar. Third prior to this,
in 1969, I had as a
policy watched my weight and took off promptly excess weight. I had gained about
20 pounds in about 6
months while in graduate school, the University of Manitoba, philosophy, in
1969-1970. Today I know that weight gain
which automatically don’t result in a subsequent reduction in appetite,
typically once the social environment which caused it has been removed, or
weight is gained in the normal environment.
Mine was the latter case. At the
time and until recently I thought my metabolism had slowed down; no I had
become insulin resistant. If my
metabolism did slow down, it was because of insulin resistance increasing
leptin which caused a reduction in my metabolic rate. I was gaining weight because
of a weight
regulator system that was malfunctioning because of insulin resistance, as explained
in 3:4, 9.
Thereafter when I gained more than 5 pound, I cut back on calories. This
is important for if the weight remains
on, the hormonal regulator system who is IR, that within 2 years the system
will reset to the new weight. If the
system is working right, thus the person is not IR, then he will not need to
diet because the system will reduce appetite.
Fourth, because of chronic back pain my doctor recommended in 1992 that
I take 2.5 grams of enteric coated aspirin.[1] Aspirin very significantly lowers blood
glucose—neither of us knew that. It also
significantly lowers the risk of cancer by over 50% at the 325 mgs daily, along
with the risk for atherosclerosis—two of the CAWD. Even at 325 to 650
mgs per day it has a
glucose lowering effect. This help to
limit, along with exercise and sport, the degree of insulin resistance. Fifth,
as mention in #8, I was aware of the
importance of hormones by the 5th decade. In 2002 at the age of 59,
fearing regulations removing of DHEA from the
market, I bought 250 mgs of DHEA. I
started taking under 20 mgs daily it
sublingually, so as to bypass the liver which would metabolize nearly all of it
on first pass from the venous portal vein.
Sixth, two-year later, at the age of 61, I was tested and had low
testosterone, sufficiently low for my doctor to prescribe topical testosterone
from a compounding pharmacy. 250 mgs daily in a lotion which yields about 25
mgs. Testosterone through its androgen
effect—and other way—lowers serum glucose, and I was a physical fitness
addict. The reduction in hormones with
age is one of the contributing factors driving the continues weight gain we
observe, must common by the 5th decade for women and 6th
form men. Their IR is progressing. The
combination of these is why I avoided the
conditions associated with the western diet, though I was unaware of the hazard
of the high sugar diet until 2013. Now
living in a gated senior community, I see a health disaster that bring a steady
flow of inner tears. I am by chance
still running at the age of 76 over 60 miles a month, and the amount of weight
I can lift is still the same, though my endurance while is about 1/3rd
of when I was 50. I certainly don’t have
the mitochondrial wellness of the Kitavans nor their low risk for CAVD, but I
am probably in the top 5% for my age group in the US. Of course that don’t
make me CAWD (bullet)
proof like the Kitavans.
Another part of my good fortune was
starting a medical website in 2004. It
has been the largest independent of industry tobacco science site on the
internet. That site exposed me to the corruption worked by insurance, corporate
clinics, and pharma, food manufacturers, tobacco[2]
and the alcoholic beverage industry.
These industries and our government makes use of the
media through social conditioning to shape behavior. The example of cigarettes
(developed
at ???)
illustrates the insidious effectiveness.
This too I missed, I’ve only owned a television for under 5 years, and
in those years it usage was limited.
Secondly my education (11 ½ years was too much a gulf for me to enjoy in
part because of education that made the mass manipulation of behavior And this
made it easy to override the media generated social condition. Profits before
people, what I call tobacco
ethics and tobacco science. I had chosen
to use a compounding pharmacy than to get 1/3rd the dose from pharma
(comparing to Androgel). The higher the
dose the greater the greater the protection from fructation—a benefit I wasn’t
aware of, though I was of the lowered risk for T2DM, see
#15. From 2004 I had been using
the lotions from a
compounding pharmacy. In 2017 Medicare
stopped covering drugs from compounding pharmacies.[3] Now I was faced with the choice of paying or
switching to a form offered by pharma. Besides lower dose, chemicals in the
patch was
a concern. The one offered in the formulary of Humana had 12
chemicals in a multi-layer patch. Given
the pattern of business, I doubted that the pharmaceutical company did honest
testing or relied upon anything other than marketing science in their selection
of chemical for their patch. Their
concern, given its complexity, was to get a patent of exclusivity, and Humana
was the spread between billing Medicare at the average wholesale price and its
cost. Low dose and chemical cocktail
decided the matter.
With my use of 325 to 650
mgs of aspirin since 1992, DHEA since 2002, and testosterone since 2004, I had
lowered IR, and by lowering IR I was raising the level of IGF-1, and lowering the rate of fructation.
It wasn’t until 2014 that I reduced sugar consumption by 80%, and at the
same time increased my ratio of fats (mainly saturated) to digestible
carbohydrates to 4 to 1. Prior to that
my sugar consumption was near the US average of about 180 pounds yearly all
sources (2:3), and by my
5th decade about 50 pounds under the national average—still well
above a safe level for my age[4]. The WHO safe level is 30 lbm a year for men
which equals 150 grams per day.[5] This brings me back to the InCHIANTI Study,
in that I had high DHEA and TTT which put me at the top of their 1st
group by 2014. Hopefully the autophagy
has repaired 70 years of the western diet, including eliminating the MTD with
significant damage to their mtDNA and replaced them with the best of my MTD.
The repair process is measured in years and won’t give me numbers like those of
the Kitavans and other LSPs (1:1).
14. Fixing the cause: If we are to
fix the problem, we must fix the cause, and this requires effective regulations
of food content, advertisement, and pricing—making unhealthy food, like with
cigarettes, more expensive. We can’t
change human behavior, we must change the environment, and thus must occur at
the top. We must blame the top for
failing to promote the public weal. The
claim of service by government is a façade, the reality is that we have a
corporatist state. Only about 2014 had I
stopped blaming the victim for obesity.
Our government must control the market place when it conflicts with the
public weal.
[1]
Neither of us knew that the coating was designed to lower serum aspirin. It
takes according to a study 8 hours for
peak level of aspirin in the blood, and total amount of absorbed aspirin is one
half that of the uncoated which reach a peak within one hour. More bad pharma
wanting illness,3:5, 6.
[2] The
blaming of cholesterol and saturated fats is another crime against billions of
people: that theory benefitted food
manufacturers and pharma and got tobacco and ethanol off the hook for the
ischemic events. Under Nixon’s
Republicans, there was a media orchestrated search for the cause of the
increase in heart attacks. Though the science had already confirmed the role of
tobacco and sugar along with refined carbs were the 2nd leading
suspect, the powers blamed on the basis of tobacco science cholesterol and
saturated fats, both of which are better than the carbs, sugar, and
polyunsaturated fats whose stock went up.
Under our corporate system we have created a health disaster world-wide
that has by percentages done more harm than any century of plagues and crop
failures as to the world wide percentage of people harmed. Historians, functioning
as historians will
write of the failure of science to serve mankind, and like the failure of
social for political reasons, the same will be written of capitalism. Or as
Adam Smith wrote, “All for ourselves,
nothing for anybody else, that is the rule maxim of the rulers of mankind,
[3]
When the media goes wild over a situation which could lead through regulations
and profits for pharma, it is a pattern repeat, serving pharma before
people. The media serves their biggest
advertise.
[4] I
had near zero soda, very low in fruit juices and drinks, and very low in table
sugar and syrups, average in ice cream, fruits, candies, and high in preserves.
[5]
This is added sugar, a defect since for some people that get that amount from
fruits and juices, and a molecule is a molecule. Once for ounce coke and
apple juice have the
same amount of sugar.
|

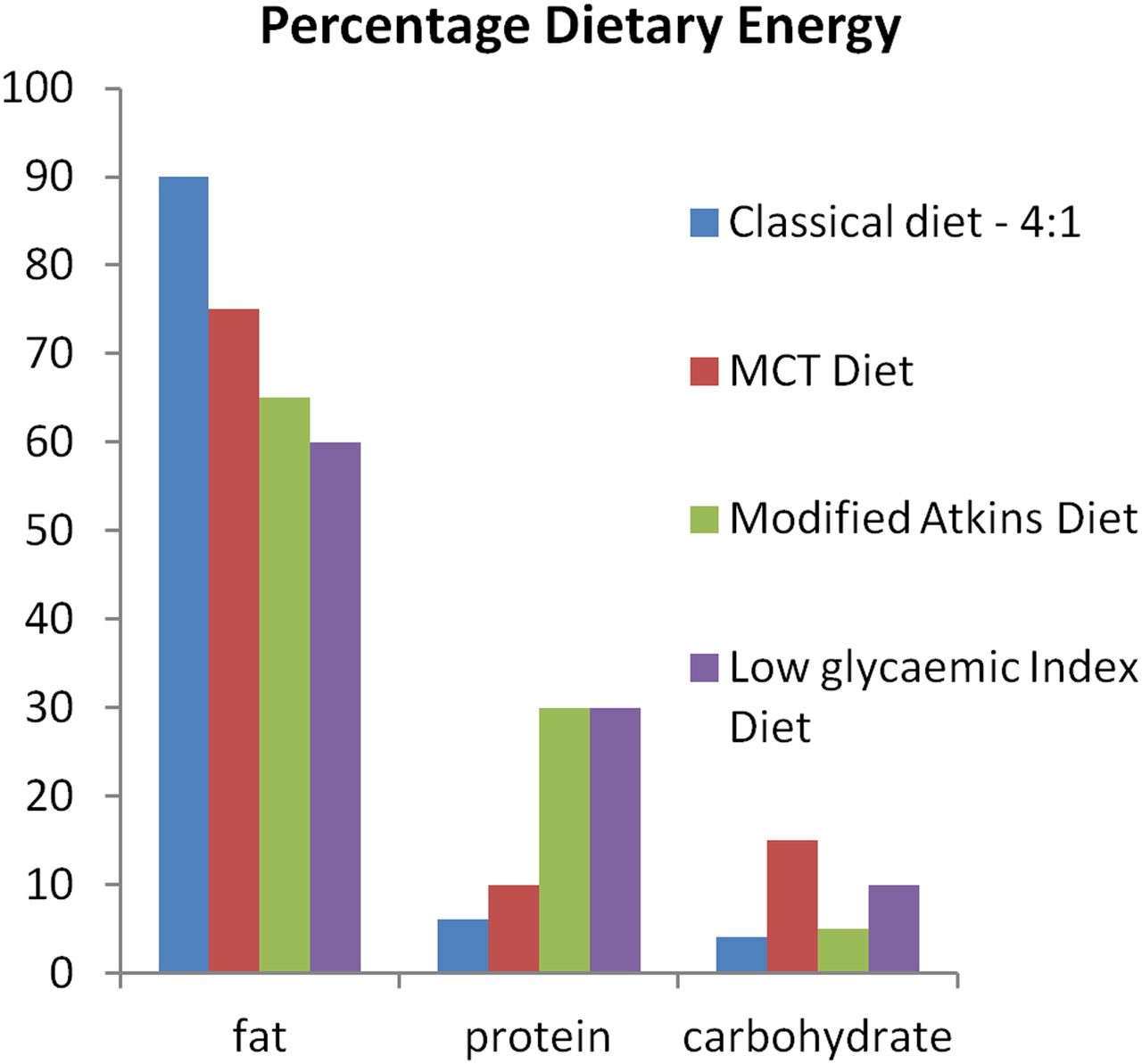
{kind=link}